Downloaded 314 times

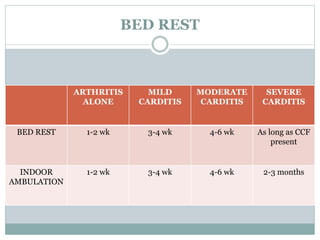
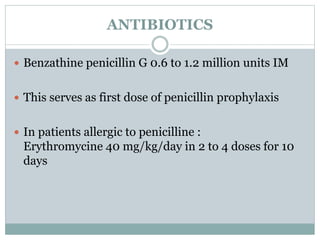
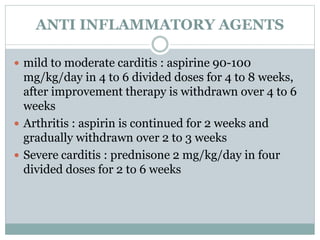
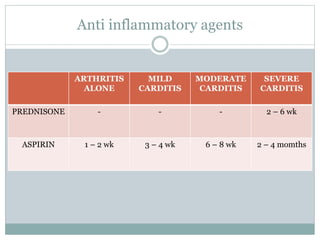
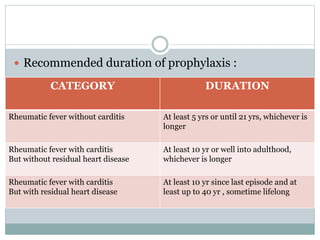

Acute rheumatic fever is an autoimmune disorder caused by an untreated streptococcal throat infection. It commonly affects children ages 5-15 and can cause long-term heart damage through inflammation of the heart valves and muscles. Symptoms include migratory joint pain, skin rashes, and involuntary movements. Treatment involves bed rest, antibiotics to treat strep, aspirin or steroids to reduce inflammation, and lifelong antibiotic prophylaxis to prevent recurrence and further heart damage. Without proper treatment and prevention, it can lead to serious and permanent heart valve problems.