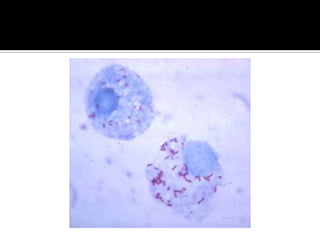
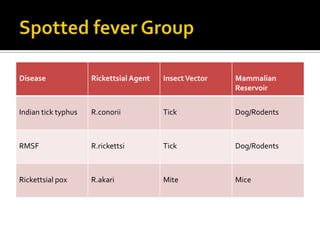
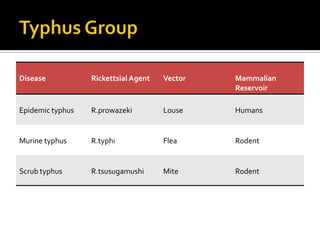
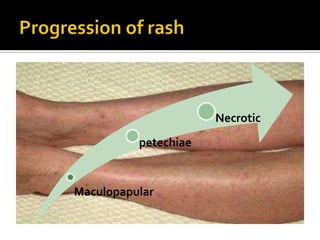
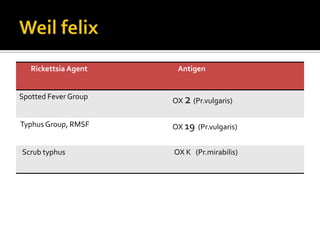
Rickettsiae are obligate intracellular bacteria that can cause diseases like Rocky Mountain spotted fever and typhus. They are transmitted through arthropod bites like ticks, mites and fleas. Common symptoms include fever, headache and rash. Diagnosis involves serologic tests detecting IgM and IgG antibodies. Doxycycline is the treatment of choice. Clinical features along with exposure history and serology can help diagnose rickettsial infections.























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




