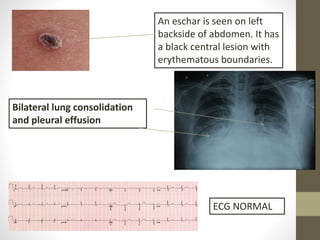
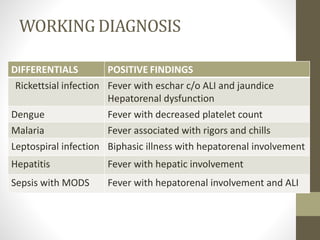
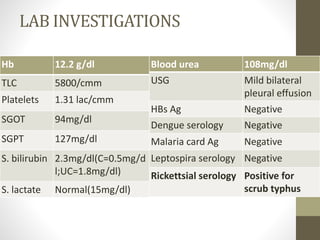
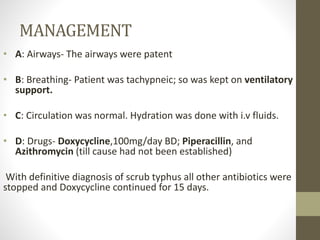
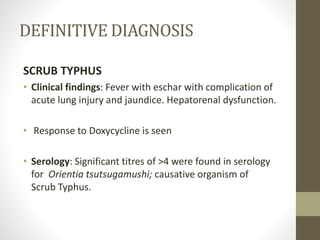
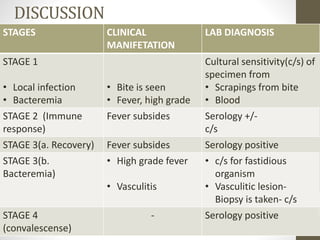
A 48-year-old male presented with 10 days of fever and 3 days of difficulty breathing. Physical examination found an eschar on his back and bilateral lung consolidation. Laboratory tests were positive for scrub typhus. He was diagnosed with scrub typhus and treated with doxycycline, which improved his condition. Scrub typhus is a rickettsial infection transmitted by chiggers that can cause fever, rash, and complications like jaundice and lung injury if not treated promptly with doxycycline.