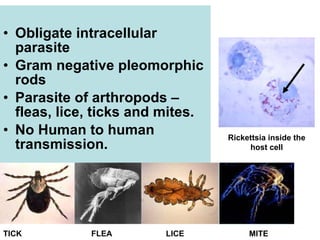
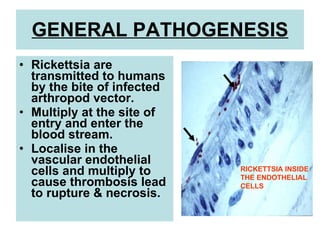
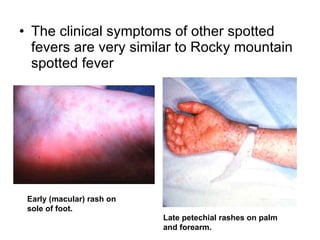
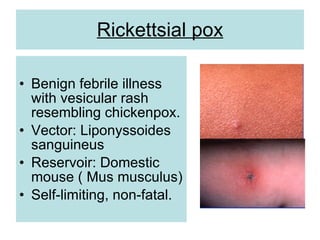
This document discusses Rickettsia, which are obligate intracellular parasites that can cause diseases like epidemic typhus, endemic typhus, and spotted fevers in humans. Rickettsia species are transmitted through the bites of arthropod vectors like fleas, lice, ticks and mites. Some key Rickettsia species and associated diseases mentioned include R. prowazekii which causes epidemic typhus, R. typhi which causes endemic typhus, and R. rickettsii which causes Rocky Mountain spotted fever. Clinical symptoms, diagnosis, treatment and prophylaxis of rickettsial diseases are summarized. Serological tests like the Weil-Felix test and immunofluorescence are used for diagnosis