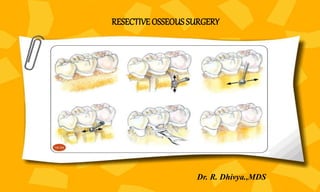
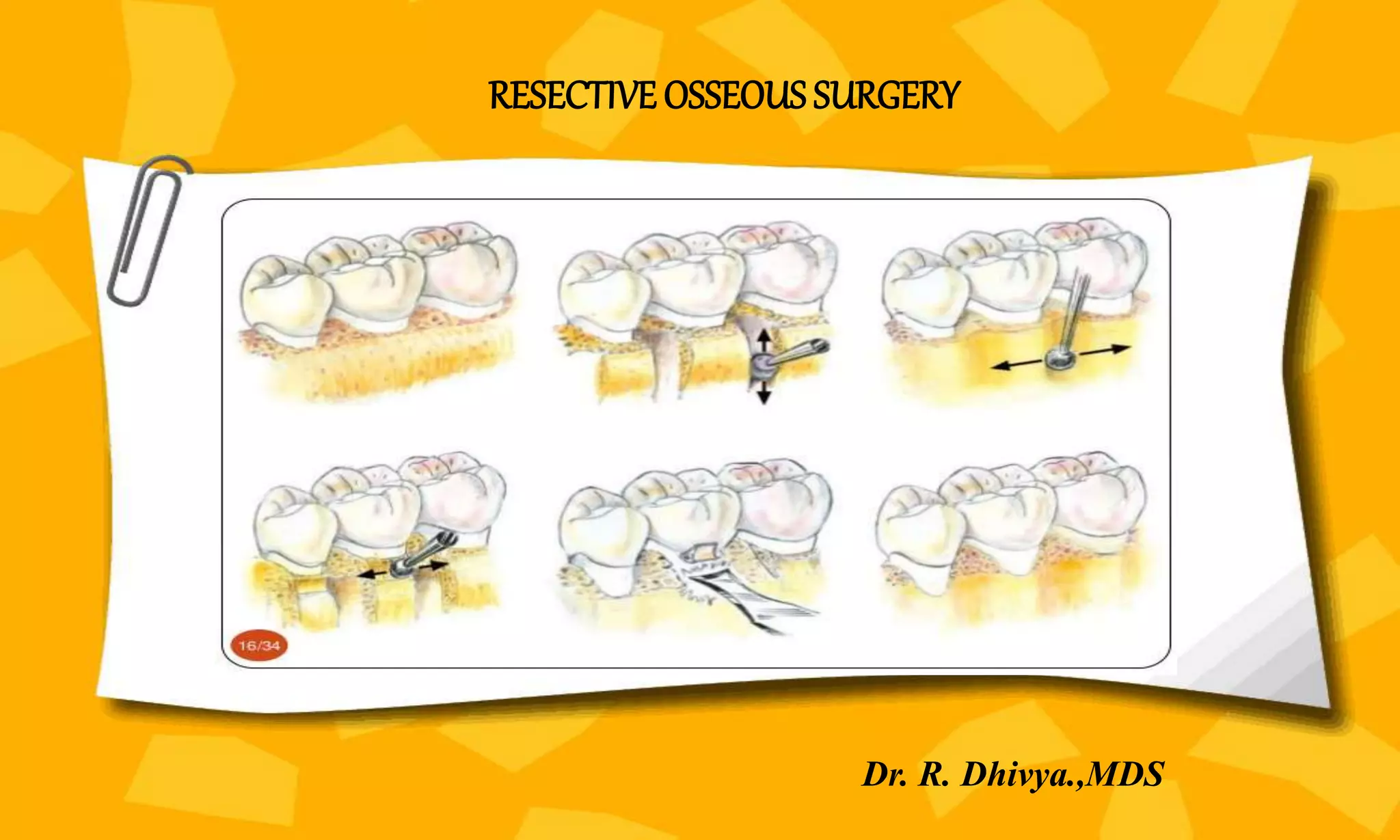
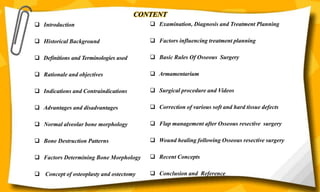

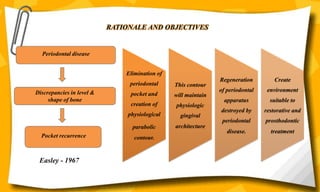











This document provides an overview of resective osseous surgery. It discusses the historical background, definitions, objectives, indications, and advantages/disadvantages of osseous surgery. It also covers normal alveolar bone morphology, bone destruction patterns in periodontal disease, and factors that determine bone morphology. Key aspects of the document include descriptions of osteoplasty, ostectomy, and the goals of resective osseous surgery to eliminate pockets and create a physiological bone contour.































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














