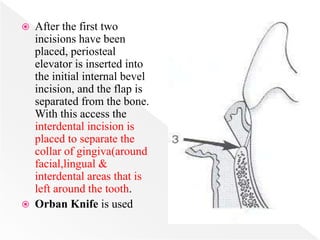
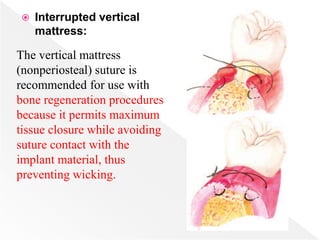
Downloaded 712 times

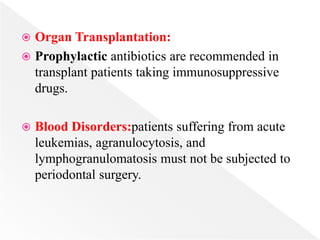

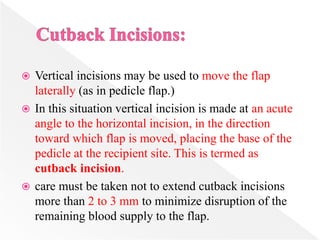


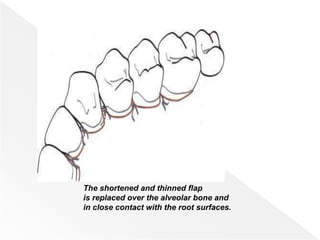


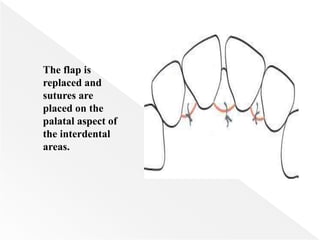
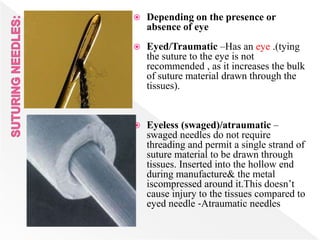
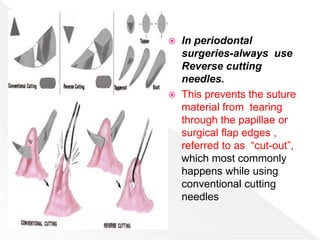
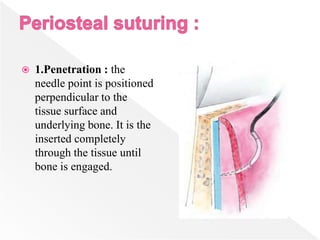
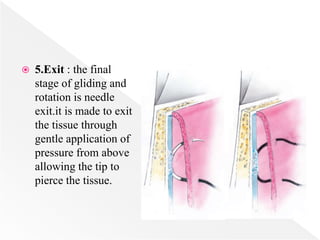
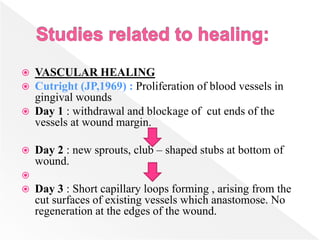
![ The suture should be placed at an equal distance
[ 2‐3 mm ] on both sides of the incision .
Suture should be always inserted through the
more mobile & from thinner flap first.
The suture should be tied so the tissue is merely
approximated & not blanched.
The knot shouldn’t be placed on the incision line
to avoid wicking effect.](https://image.slidesharecdn.com/wkg0vwm1qkofuxihhuw8-signature-b52533d3448a3f76135ecce1dabba3dd8bfcdcaa2417ed9a5427ef6da18fff4c-poli-170303191506/85/Principles-of-flap-surgery-copy-173-320.jpg)
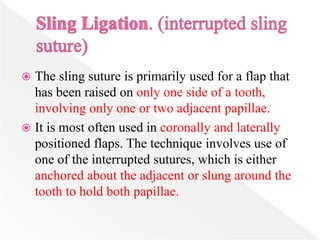





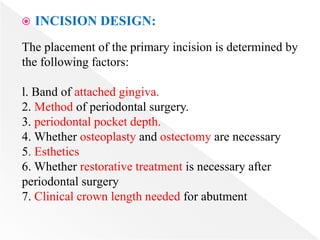
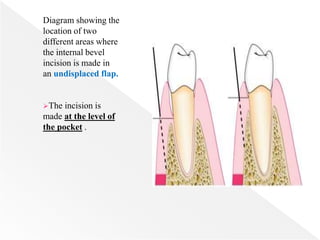
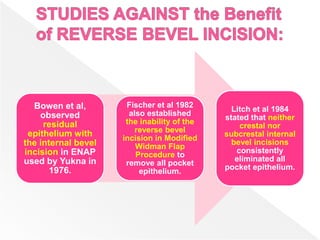
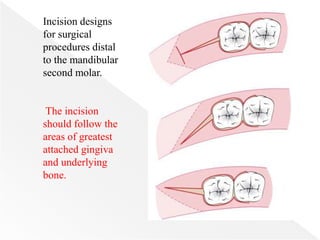
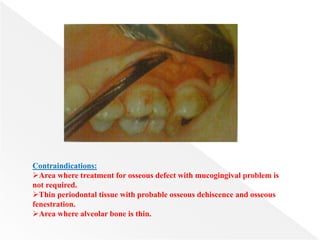
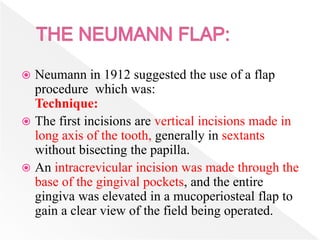
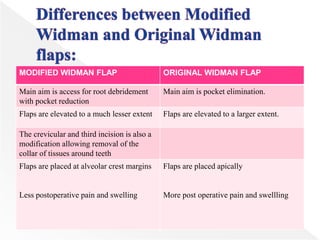
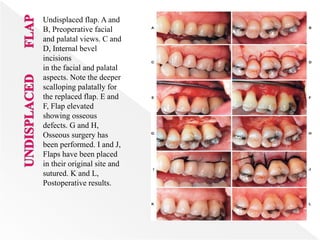
1. Periodontal therapy aims to establish a healthy dentition through non-surgical and surgical treatment. Surgical treatment often involves raising a periodontal flap to access the root surface. 2. There have been many advances in periodontal flap design since the 19th century aimed at improving access, visibility and outcomes. Factors such as blood supply, extent of disease, osseous defects and esthetics inform the choice of flap. 3. Modern periodontal flap surgery techniques emphasize preserving blood supply through careful incision placement, minimizing trauma, and obtaining adequate access and closure.











![Wound healing [including healing after periodontal therapy]](https://cdn.slidesharecdn.com/ss_thumbnails/woundhealingjr-150516123855-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)


























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















