





































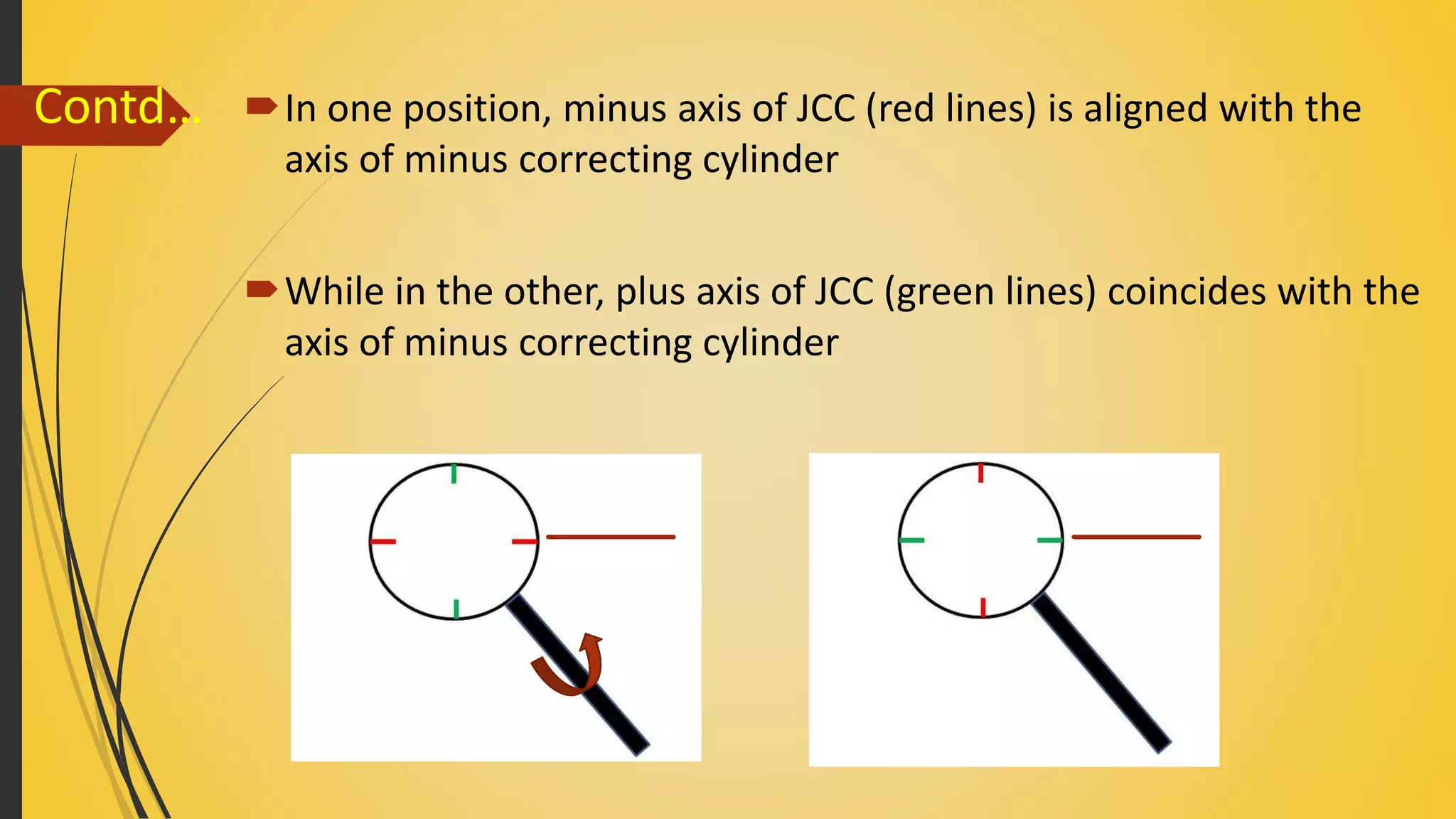




















1) The document discusses subjective refraction techniques for astigmatism, including determining the spherical and cylindrical corrections. 2) Key steps include controlling accommodation, finding the monocular best sphere using VA or bichrome tests, and determining the cylindrical component using fogging with targets like clock dials or Jackson cross cylinders. 3) The axis of the cylindrical correction must match the axis of the patient's astigmatism to fully correct their refractive error.












































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










