


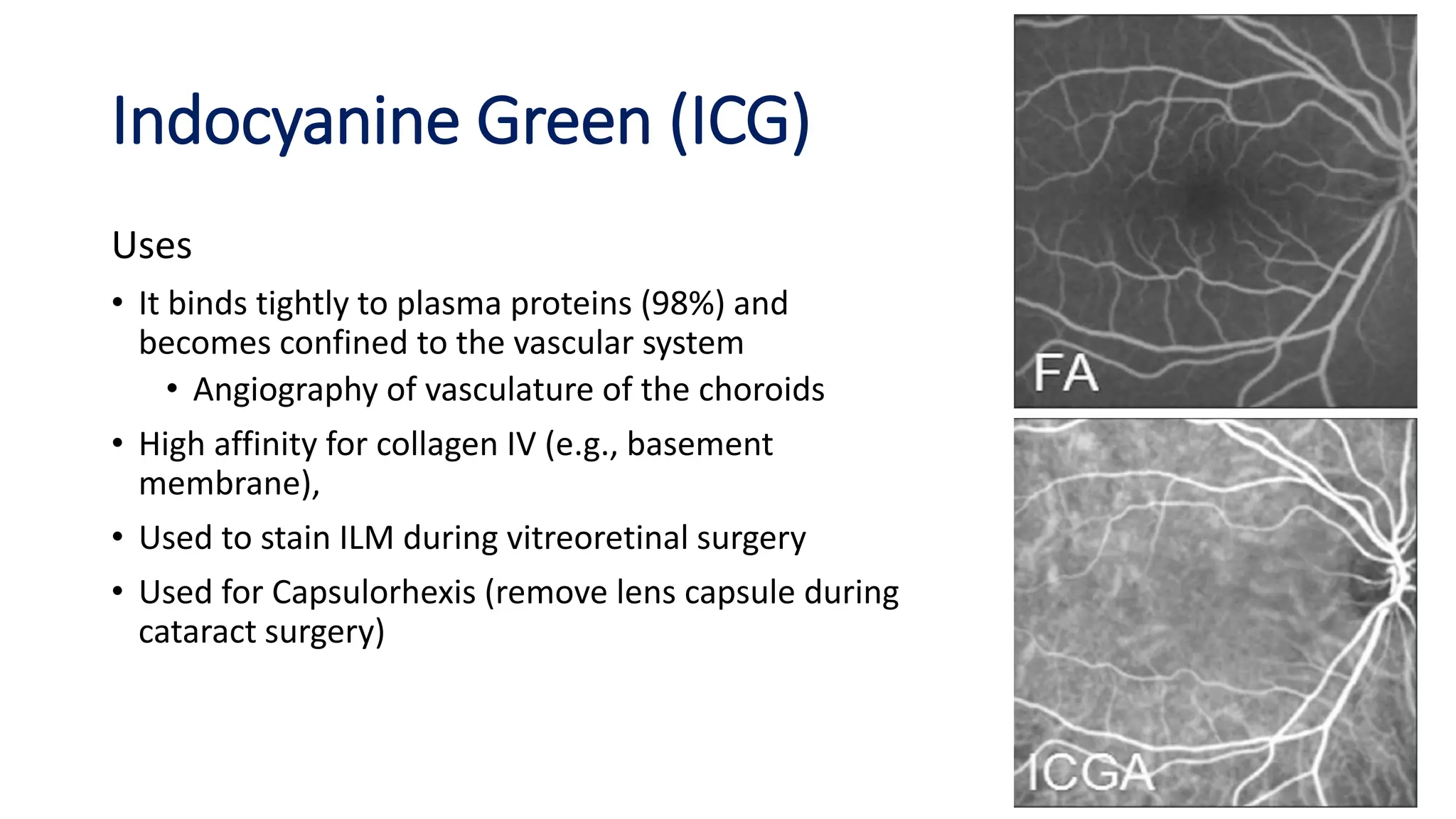
![Indocyanine Green (ICG)
Concentration
• 40mg in 2ml for IV injections
• 0.05% to 0.5% for posterior segment
surgeries, e.g., ILM [internal limiting
membrane] staining, the anterior capsule
stain in cataract surgeries
Properties
• It is a cyanine dye used for ophthalmic
angiography
• It has a peak spectral absorption at infrared
frequencies of 805 nm.
• Excretion: liver and bile](https://image.slidesharecdn.com/8-240329060914-626e35a5/75/Vital-dyes-and-stains-Used-in-Ophthalmic-Practice-pptx-16-2048.jpg)
![Trypan blue
Concentration
• Anterior capsular staining and enucleation surgery for Tenon's capsule - 0.06 %
• Posterior segment surgeries - 0.15%
Properties
• This stains mucus and dead cells which have undergone structural changes
• The dye does not penetrate the capsule, permitting visualization of the anterior
capsule in contrast to the non-stained lens cortex and inner lens material.
• Selectively stains the Tenon's capsule, and hence is used after enucleation surgeries
during layered closure, without entrapment of conjunctiva in the Tenon's capsule.
• In the posterior segment of the eye, it stains ERM [epiretinal membrane] blue on
instillation after fluid/air exchange](https://image.slidesharecdn.com/8-240329060914-626e35a5/75/Vital-dyes-and-stains-Used-in-Ophthalmic-Practice-pptx-19-2048.jpg)



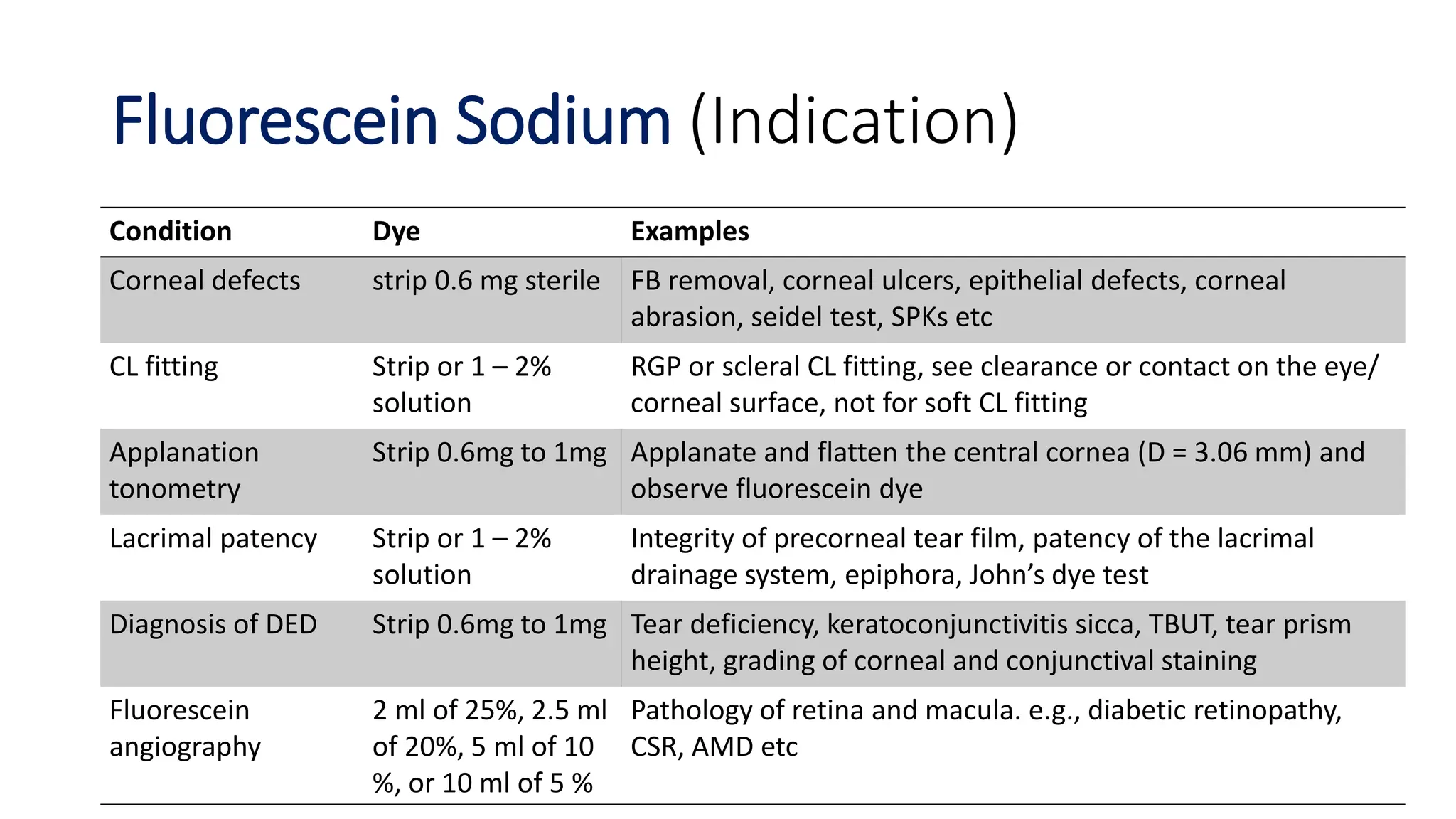
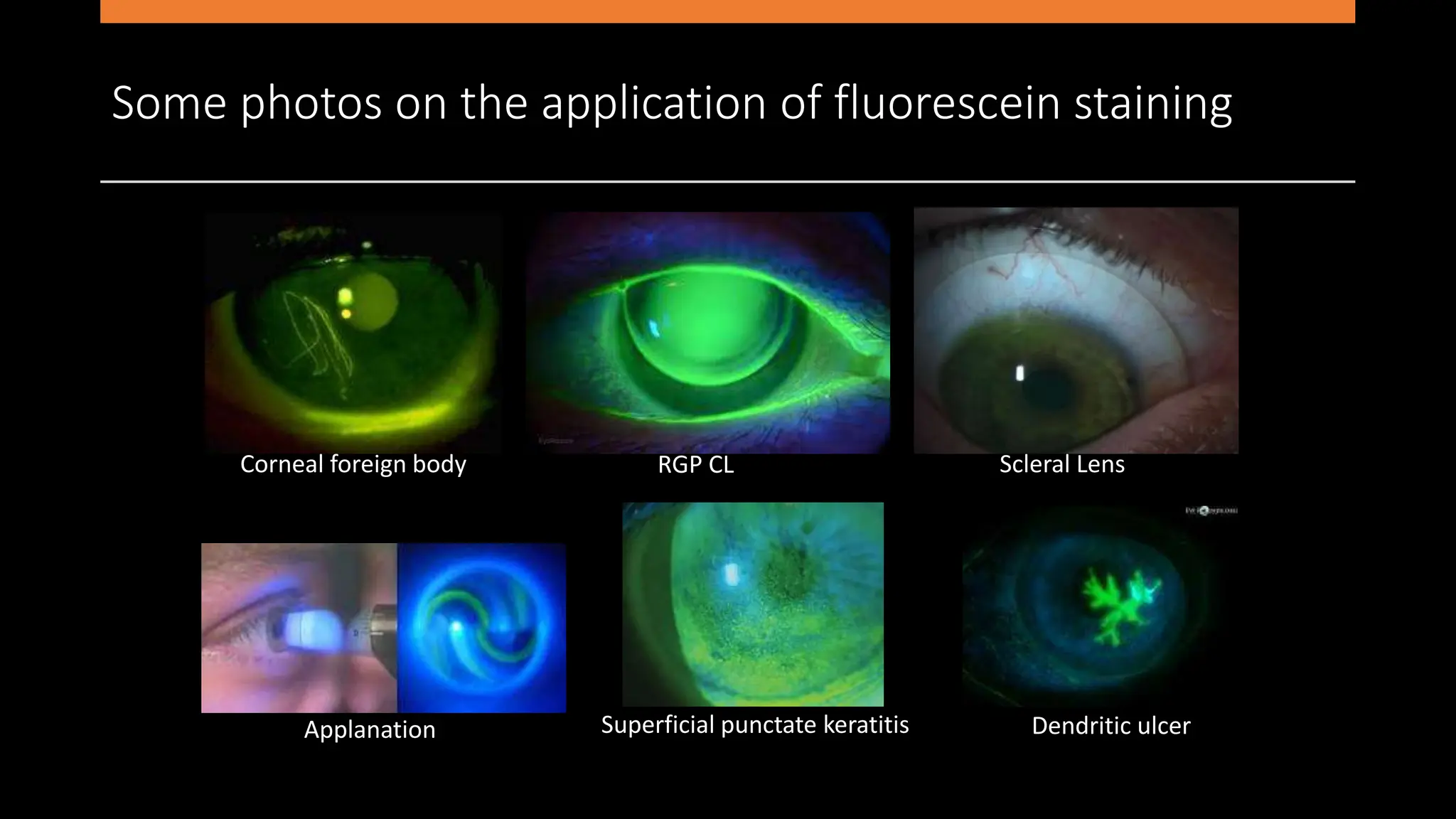
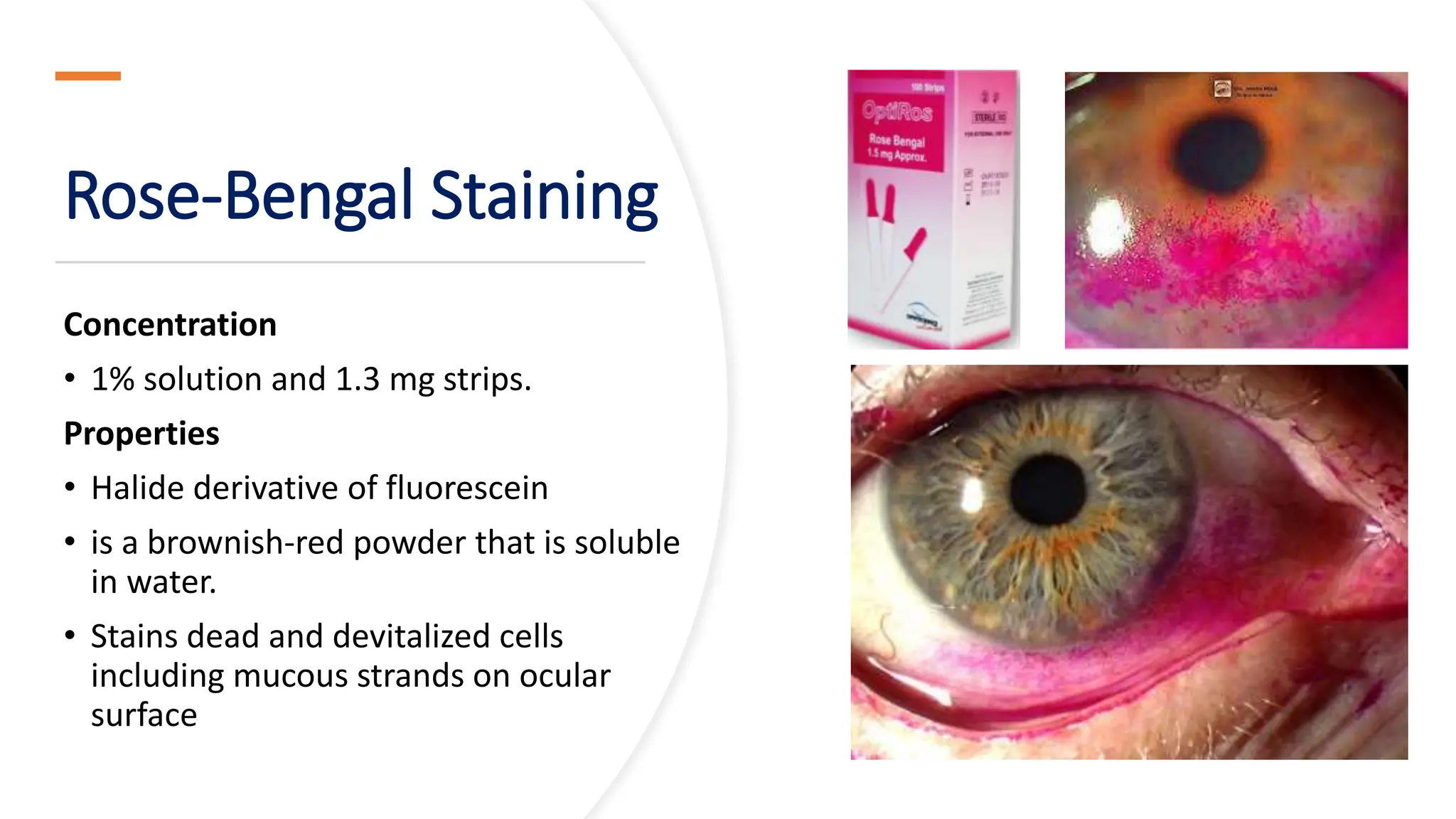
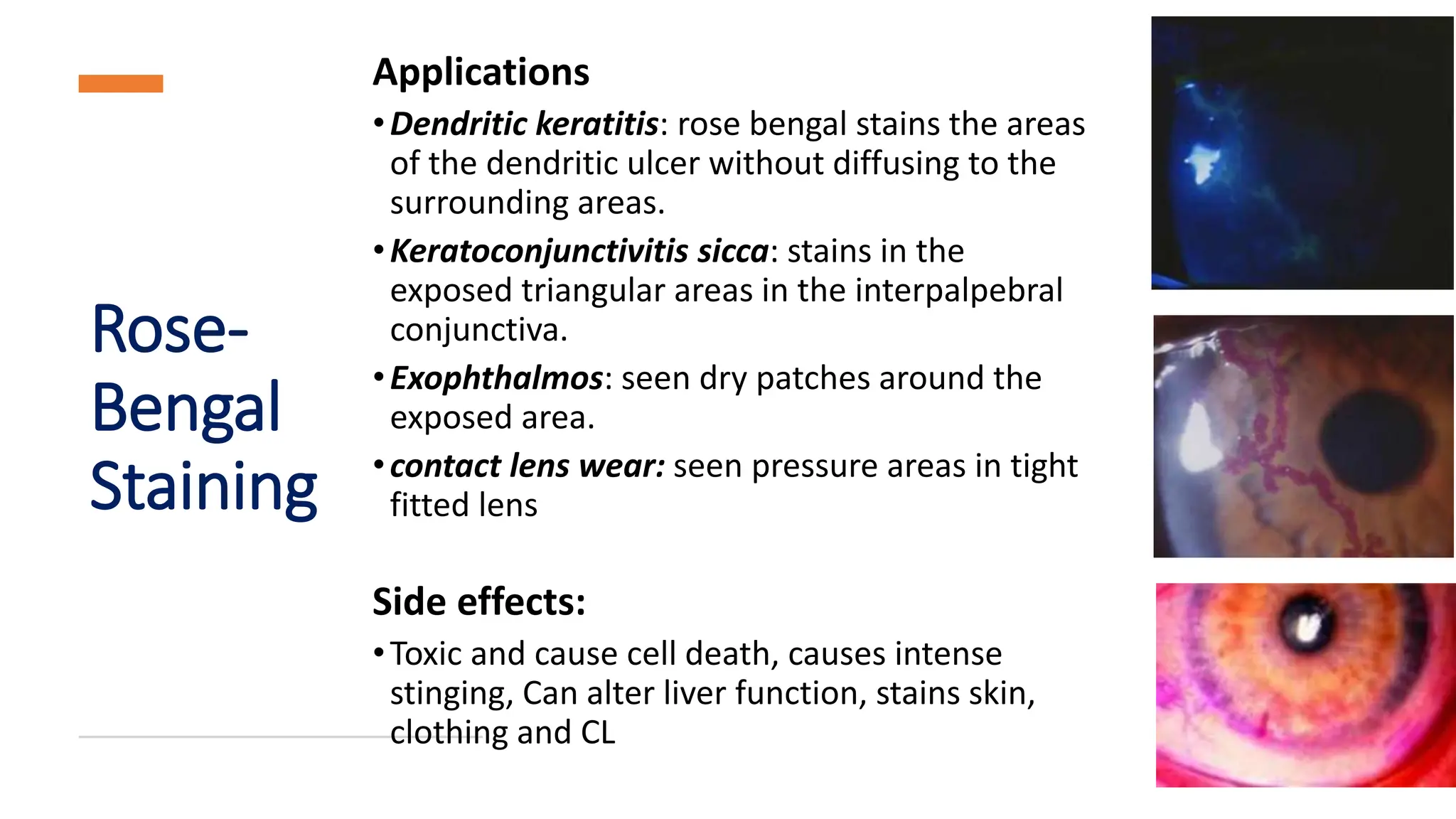
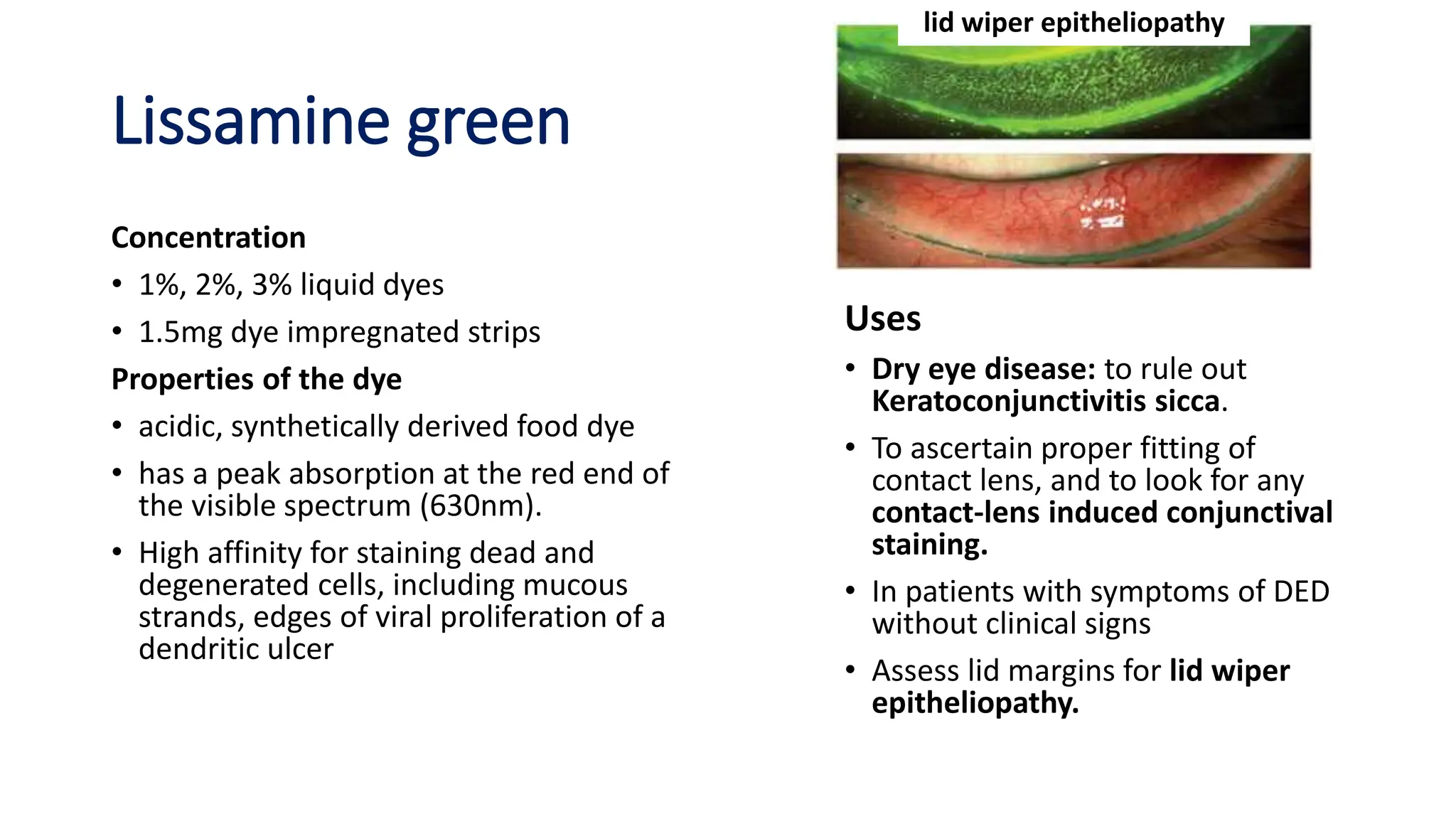
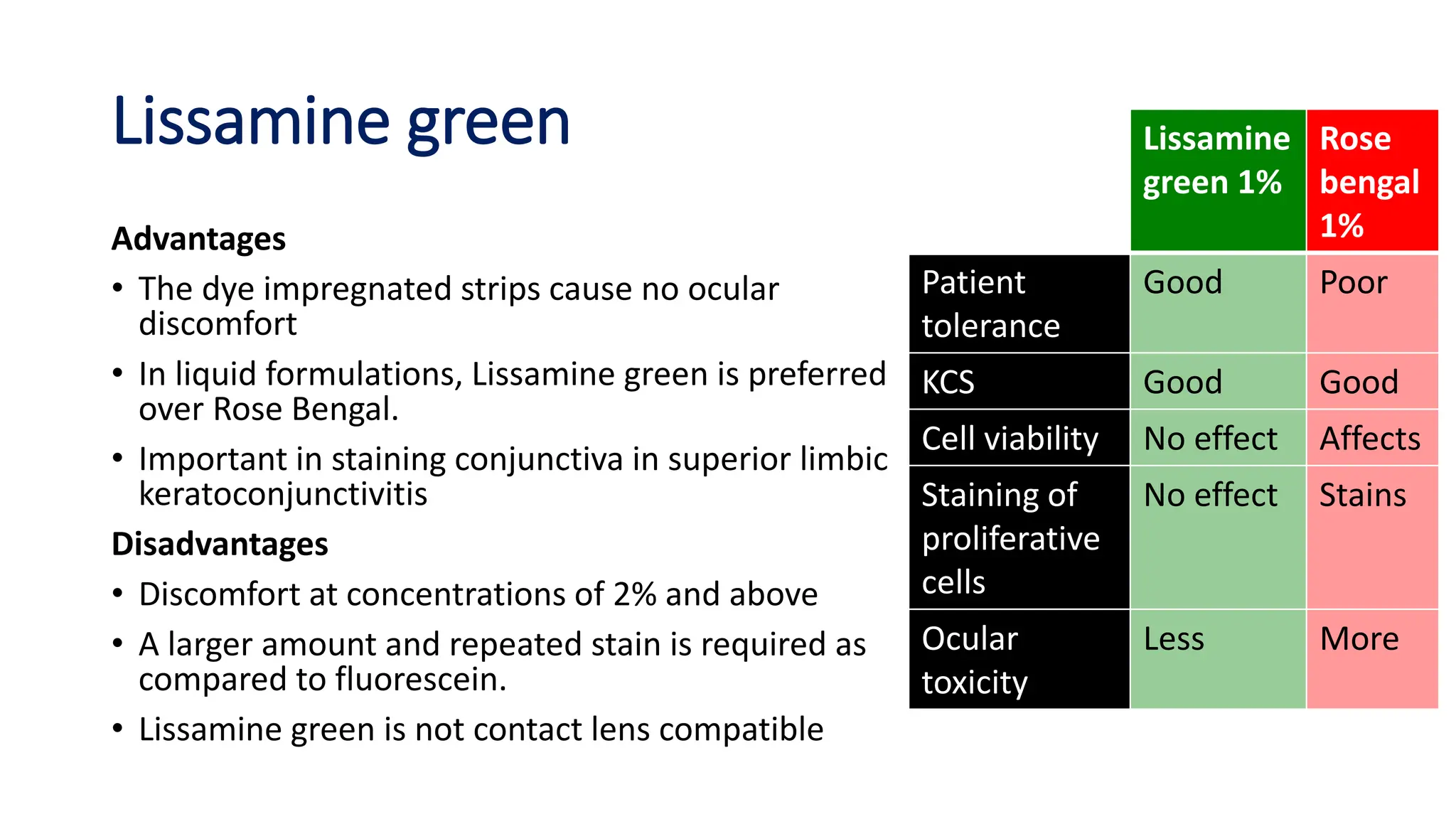
Vital dyes are used in ophthalmology for diagnostic purposes without pharmacological effects. Common vital dyes include fluorescein sodium, rose bengal, lissamine green, methylene blue, indocyanine green, and trypan blue. Each dye has unique absorption and fluorescence properties that allow them to selectively stain tissues or structures in the eye. The dyes are used to detect defects on the ocular surface, assess tear film and lacrimal drainage, and aid in a variety of surgical procedures. Potential side effects vary between dyes and include irritation, staining of other tissues, and toxic reactions.























































































