
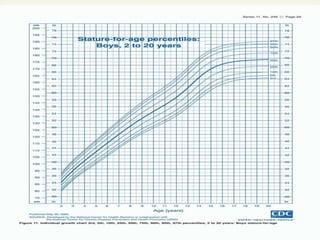


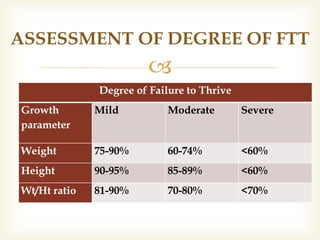

Failure to thrive (FTT) refers to inadequate growth in infants and children. It is defined as weight below the 3rd percentile or a significant decrease from an established growth curve. FTT can be organic, due to medical causes like prematurity or malnutrition, inorganic, due to non-medical causes like neglect or poor parenting, or mixed. Clinical features include low weight and height compared to standards, as well as decreased developmental milestones. Diagnosis involves medical history, physical exam, and tests to identify underlying causes. Management focuses on optimizing nutrition, providing a nurturing environment, parental education, and treating any medical issues contributing to FTT.






















































































