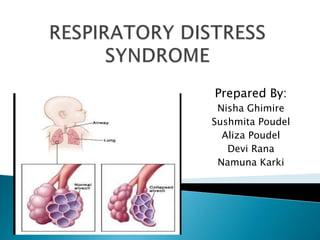
Respiratory distress syndrome is a condition in premature infants caused by a lack of surfactant in the lungs. Surfactant is needed to keep the alveoli open during breathing. Without it, lungs collapse during exhalation due to surface tension. This causes respiratory failure. Risk factors include prematurity, meconium aspiration, or maternal complications. Diagnosis involves assessing breathing rate, lung sounds, oxygen needs and chest x-rays. Treatment focuses on providing oxygen, medications, and supportive care until the lungs mature enough to produce surfactant.
Every year more than 10 million children die in developing countries due to acute respiratory infections (mostly pneumonia), diarrhea, measles, malaria, or malnutrition - and often to a combination of these illnesses. In 1990s, the WHO, in collaboration with UNICEF and many other agencies, institutions and individuals, responded to this challenge by developing a strategy known as the Integrated Management of Childhood Illness (IMNCI).This strategy adopted in India as Integrated Management of Neonatal and Childhood Illness (IMNCI). IMNCI caters to two groups of children
• 0-2 months, referred to as young infants.
• 2 months to 5 years, referred to as children.
neonatal hypothermia is a very emergency condition. if we identify this in early stage we can save the life of neonate. all should know about the maintaining the temperature if the neonate is in our home.
Every year more than 10 million children die in developing countries due to acute respiratory infections (mostly pneumonia), diarrhea, measles, malaria, or malnutrition - and often to a combination of these illnesses. In 1990s, the WHO, in collaboration with UNICEF and many other agencies, institutions and individuals, responded to this challenge by developing a strategy known as the Integrated Management of Childhood Illness (IMNCI).This strategy adopted in India as Integrated Management of Neonatal and Childhood Illness (IMNCI). IMNCI caters to two groups of children
• 0-2 months, referred to as young infants.
• 2 months to 5 years, referred to as children.
neonatal hypothermia is a very emergency condition. if we identify this in early stage we can save the life of neonate. all should know about the maintaining the temperature if the neonate is in our home.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
2. The term respiratory distress
syndrome are most often applied to
the severe lung disorder in neonate
which is primarily related to lung
immaturity.
It is responsible for more infants
death and neurological complications.
3. Respiratory distress syndrome is a
syndrome of premature neonates that
is characterized by progressive and
usually fatal respiratory failure
resulting from atelectasis and
immaturity of lungs.
It was formerly known as Hyaline
membrane disease.
4. The breathing rate is usually more than
60 breaths per min and/or use of
accesory muscle of respiration which
maybe accompanied by grunting.
Surfactant production starts around
20wks of life and peaks at 35wks .
Therefore any neonate less than 35 wks
is prone to develop RDS, without
surfactant infants are unable to keep
their lungs inflated.
8. Non- pulmonary risk factors :
Sepsis
Cardiac defect
Exposure to cold
Hypoglycemia
Metabolic acidosis
Acute blood loss
9. In RDS, the basic abnormality is
surfactant deficiency. It is lipoprotein
containing phospholipids produced by
type II alveolar cells of lungs and helps
to reduce surface tension in alveoli.
11. During inspiration,
More negative pressure is needed
to keep alveoli patent.
Due to all these conditions,
Inadequate Oxygenation
Increased work of breathing
Hypoxemia and acidosis
13. Tachypnea (< or = 80 – 120 breaths
per min) [Wong’s]
Dyspnea
Pronounced intercostals or substernal
retractions
Fine inspiratory crackles
Audible expiratory grunt
Flaring of external nares
Cyanosis or pallor
14. Manifestation as the disease progress
Apnea
Flaccidity
Absent spontaneous movement
Unresponsiveness
Diminished breath sound
Mottling
In severe condition – shock like state
15.
16. History taking
Physical examination
Chest x-ray :ground glass appearance
ABG
Pulse oxymetry
Pulmonary function test
Shake test
Downe’s score
17.
18. SHAKE TEST :
It can be done on the
gastric aspirate to determine lung
maturity.Mix 0.5 ml of gastric aspirate
with 0.5 ml of absolute alcohol in a
test tube and shake for 15 sec.
Formation of bubbles indicate
adequate surfactant and less chance
of RDS.
19. DOWNE’S SCORE:
Score 0 1 2
Respiration
(rate/min)
<60 60-80 >80 or
apnea
Cyanosis Nil in room
air
+nt in 40 %
oxygen
+nt in >40%
oxygen
Retraction none Mild Moderate to
severe
Grunting None Audible with
sthethescope
Audible
without
stethescope
Air entry Clear Delayed or
Decreased
Barely
audible
20. Total score in normal infant: 0
Mild: 1 – 3
Moderate : 4 – 6
Severe : 7 - 10
21. MEDICAL MANAGEMENT
Neonates suspected to have RDS need
to be treated in NICU.
Administer IV fluids and oxygen .start
oxygen therapy @4-6 lit/min.
Maintain oxygen saturation between
90-95%.
Administration of exogenous
surfactant through ET tube directly
into trachea.
22. Medicines:
Antibiotics : aminoglycosides, amoxicillin ,
ampicillin , cotrimoxazole and procaine
penicillin usually given for 7-10 days.
Muscle relaxants : pancuronium
Diuretics: furosemide
Antacids : sodium bicarbonate, sodium citrate
Indomathacin : if patent ductus arteriosus
23. Supportive management :
Maintain adequate hydration and
electrolyte status.
Administer anti pyretics to reduce
fever.
Maintain acid base balance.
No nipple or gavage feeding : increase
respiratory rate and chance of
aspiration.
IV line for fluid/hydration,nutrition
and medication.
25. Nursing diagnosis:
Ineffective breathing pattern related to
surfactant deficiency and alveolar
instability.
Impaired gas exchange related to
immature pulmonary function.
Altered nutriton :less than body
requirement related to feeding
difficulties.
26. Altered body temperature related to
prematurity.
Parental anxiety related to disease
condition.
Risk for injury (brain injury)related to
hypoxemia.
27. Nursing interventions:
Assess pre-term infant for respiratory
and general status :oxygen saturation
,cyanosis , ABG, axillary temperature,
respiratory pattern
Maintain airway and administer
oxygen @4-6 lit/min.
Provide ventilatory support in case of
need.
28. Perform gentle chest percussion,
vibration and postural drainage based
on assessed need and infant
tolerance.
Monitor for signs of hyperthermia
(flushing,tachycardia, altered level of
consciousness) and hypothermia
(decreased activity, respiratory
distress deterioration, cool mottled
extremities)
29. Place the infant in radiant warmer ,
incubator.
Use environmental control : warm
cloths warm, well ventilated room etc
for decreasing heat loss.
Position the infant to facilitate open
airway on the side with head
supported in aliment by a small
folded sheet (SMITING POSITION).
30. Quick gentle suctioning (not more
than 5 sec)with fine catheter as
needed.
Maintain neutral thermal environment
to decrease metabolic requirement
and to conserve oxygen utilization.
Maintain parenteral nutrition , avoid
oral feeding or through tube if child is
in distress.
31. Maintain optimal nutrition pattern of
infant
Once baby is breathing without
distress NG feeding is started.
Involves parent in the care of children
and allow frequent visit to encourage
and promote infant – parent bonding.
32. Skin care with frequent position
change.
Mouth care.
Psychological support and provide
adequate information about child’s
condition.