Downloaded 6,003 times





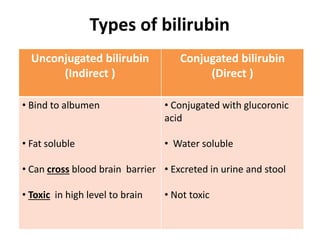
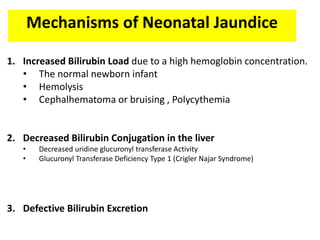










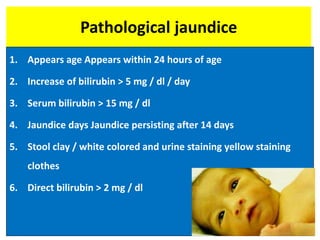





















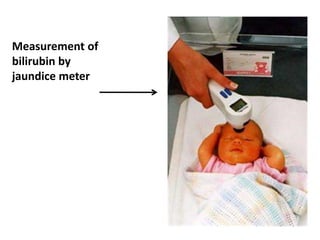






















Neonatal jaundice is a common condition that requires medical attention in newborns. It is caused by high levels of bilirubin, which is produced from the breakdown of red blood cells. There are two main types - physiological jaundice, which appears after 24 hours and is harmless, and pathological jaundice, which can be a sign of other health issues and sometimes requires treatment. Pathological jaundice has various potential causes, including blood group incompatibility, infections, or liver problems. Treatment depends on the underlying cause and severity of jaundice, and may involve phototherapy, intravenous immunoglobulins, or exchange transfusions in severe cases to prevent potential brain damage from high bilirub






















































































