Download as PPSX, PPTX
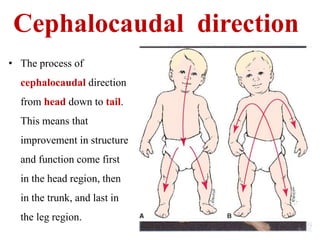
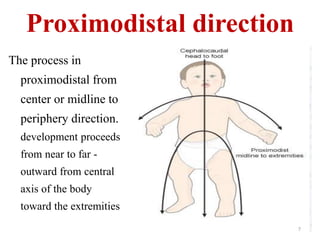








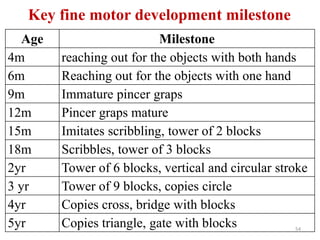
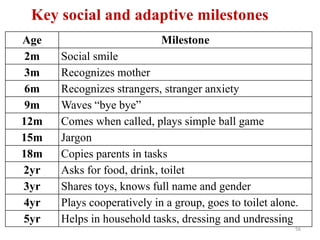
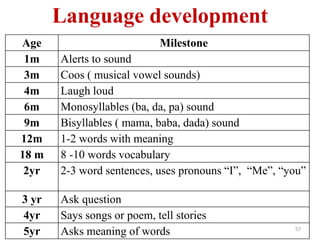



The document discusses growth and development in children. It defines growth as a quantitative increase in body size through cell multiplication, while development is the qualitative functional and physiological maturation of an individual. The principles of growth include cephalocaudal development from head to tail, proximodistal development from center to extremities, and general to specific development from broad abilities to fine motor skills. Factors that influence development are genetic, prenatal such as maternal health, and postnatal including nutrition, environment and socioeconomic status. The document outlines assessments of physical growth parameters and developmental milestones.