Downloaded 369 times

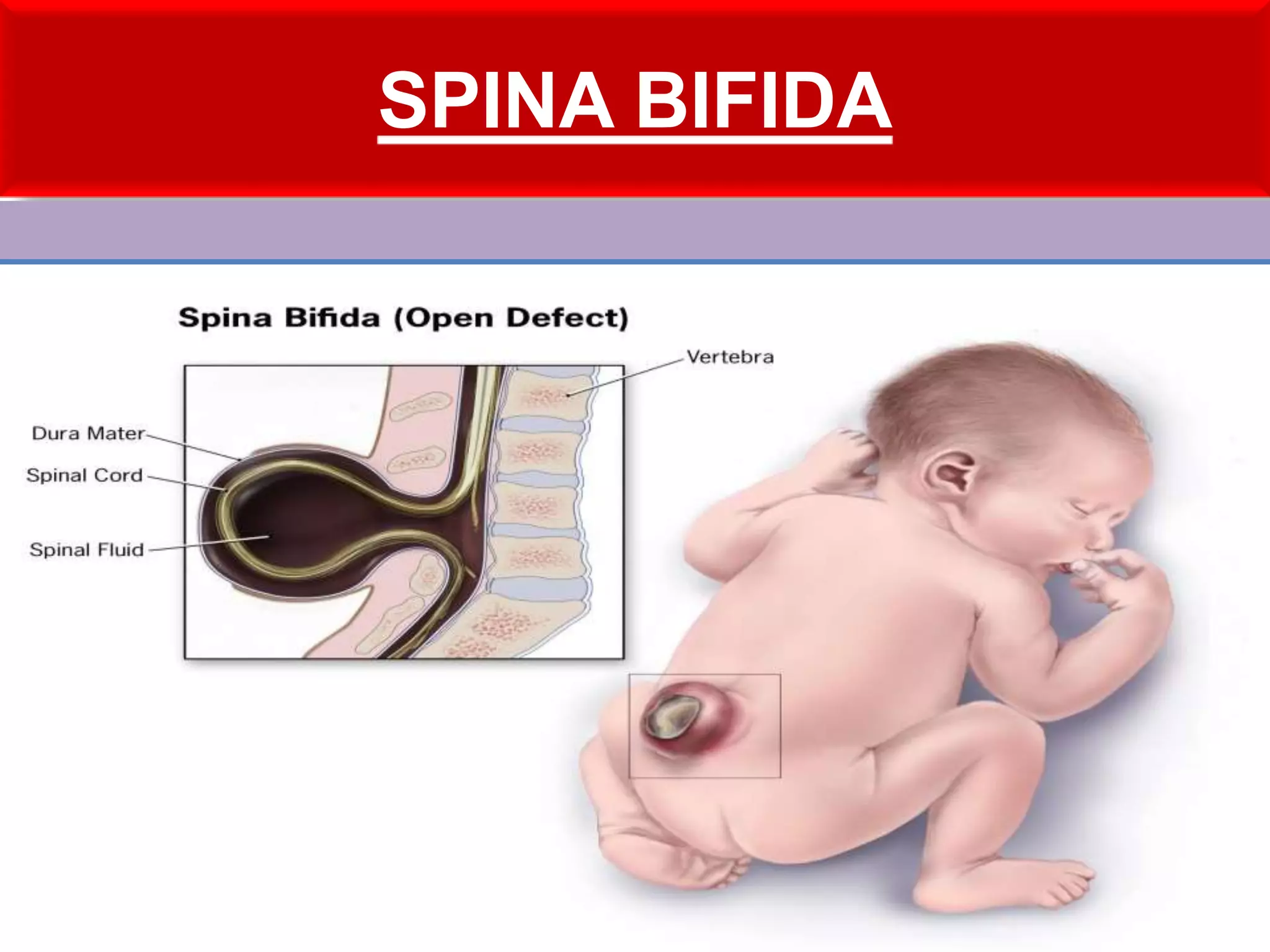
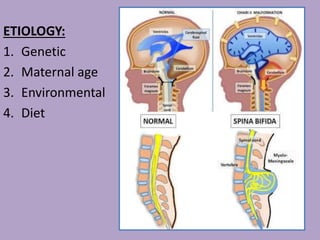
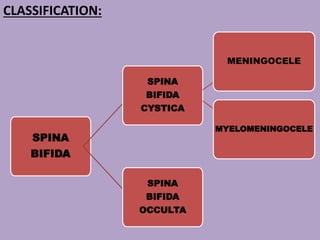
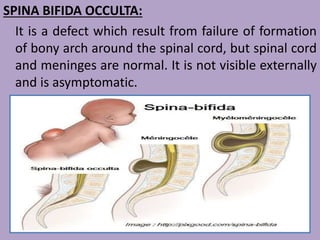
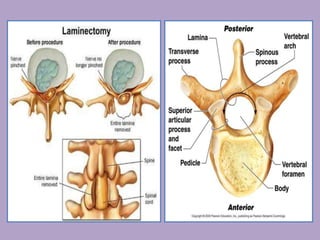


Spina bifida is a birth defect where the spine and spinal cord do not form properly, leaving an opening in the spine. It occurs in about 1-2 per 1000 live births. There are three main types: spina bifida occulta which has no symptoms, meningocele which is a sac protruding from the spine containing fluid and membranes, and myelomeningocele which is the most severe form where the spinal cord and membranes protrude out. Treatment depends on the type but may include surgery to close the opening after birth along with management to prevent infections and complications.























































































