Downloaded 503 times

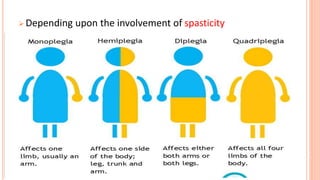
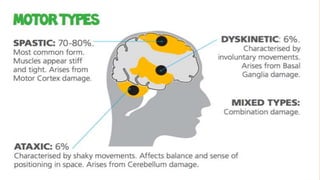


Cerebral palsy is an umbrella term for physical disabilities caused by damage to the brain before or at birth. It is characterized by impaired muscle coordination and other disabilities. The prevalence is about 4 per 1000 live births. There are several types classified by motor deficit, including spastic (the most common), dyskinetic, atonic, and mixed forms. Management involves medical treatment to alleviate symptoms, physical and occupational therapy, and sometimes surgery to correct issues like scoliosis.