Downloaded 5,908 times

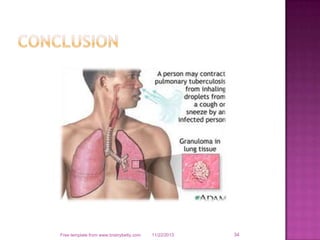

Tuberculosis is a chronic bacterial infection caused by Mycobacterium tuberculosis that primarily affects the lungs. It spreads through inhaling droplets from an infected person and can spread to other parts of the body. Symptoms include cough, weight loss, fever and night sweats. Diagnosis involves chest x-ray, sputum culture and tuberculin skin test. Treatment requires taking multiple antibiotics daily for 6-12 months under direct observation to prevent drug resistance and cure the infection.





































































































