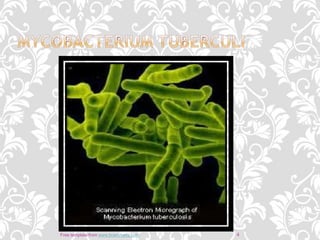
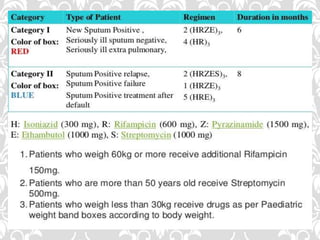
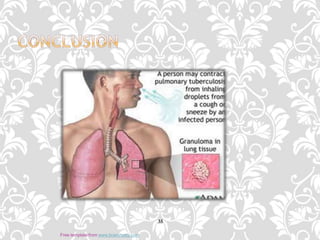
Tuberculosis is a bacterial infection that primarily affects the lungs and is spread through inhaling droplets from infected individuals. It is a global health problem that kills over 5,000 people per day. Risk factors include immunocompromised status, drug/alcohol abuse, lack of healthcare, and living in close quarters with an infected individual. Symptoms can include cough, weight loss, fever, and night sweats. Diagnosis involves tests of sputum, skin, blood, and imaging. Treatment requires a multi-drug regimen over a period of 6-12 months under direct observation to prevent drug resistance.





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












