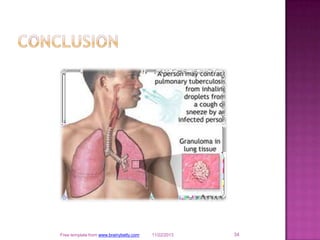
Tuberculosis is a bacterial infection that is spread through inhaling droplets from an infected person when they cough or sneeze. It primarily affects the lungs but can spread to other organs. Symptoms include cough, weight loss, fever and night sweats. Diagnosis involves tests like chest x-rays, sputum smears and TB skin tests. Treatment requires taking multiple antibiotics daily for 6-12 months to prevent drug resistance and cure the infection. Strict treatment adherence is important to reduce the spread of this globally prevalent disease.


































![TB [Autosaved].pptx gg897dt4sr3rshtfjry8](https://cdn.slidesharecdn.com/ss_thumbnails/tbautosaved-241204074724-e0f6b93a-thumbnail.jpg?width=640&height=640&fit=bounds)

![TB [Autosaved].pptxnhgfytetrstrht65356yf](https://cdn.slidesharecdn.com/ss_thumbnails/tbautosaved-241207141258-e6d69ce6-thumbnail.jpg?width=640&height=640&fit=bounds)









































