Downloaded 43 times
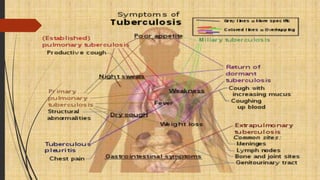
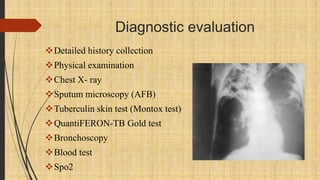
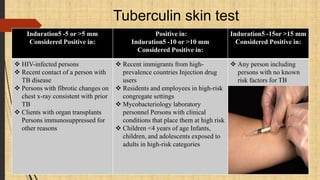
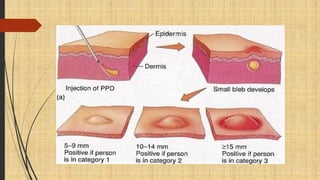

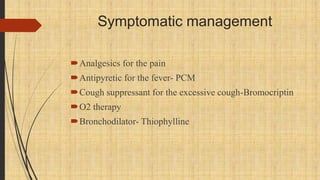


Tuberculosis is an infectious disease primarily affecting the lung parenchyma caused by Mycobacterium tuberculosis. Risk factors include age, immune status, living conditions, and country of origin. It spreads through airborne droplets from coughing, sneezing, etc. Symptoms may include cough, fever, weight loss, and night sweats. Diagnosis involves chest x-ray, sputum smear, tuberculin skin test, and culture. Treatment involves a combination of antibiotic medications over several months. Patient education focuses on medication compliance, prevention of spread, signs of treatment failure, and lifestyle modifications.