Downloaded 747 times
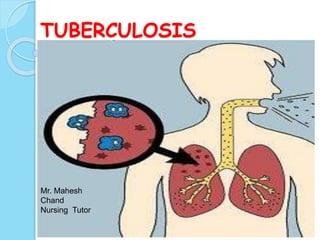

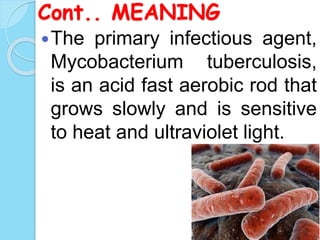
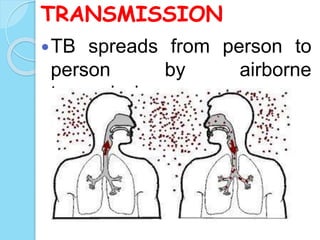


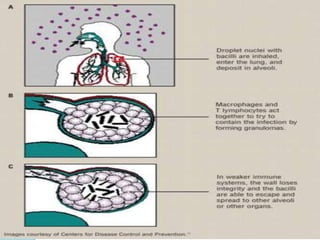







Tuberculosis is a worldwide public health problem caused by the bacterium Mycobacterium tuberculosis. It primarily affects the lungs but can spread to other organs. Major risk factors include close contact with an active case, immunocompromised status, and living in crowded conditions. TB progresses through primary, latent, and active stages. Treatment involves a multi-drug regimen administered under direct observation for 6-12 months. Complications may include spread to other organs. Nursing care focuses on airway clearance, treatment adherence, nutrition, and preventing spread.























































































