










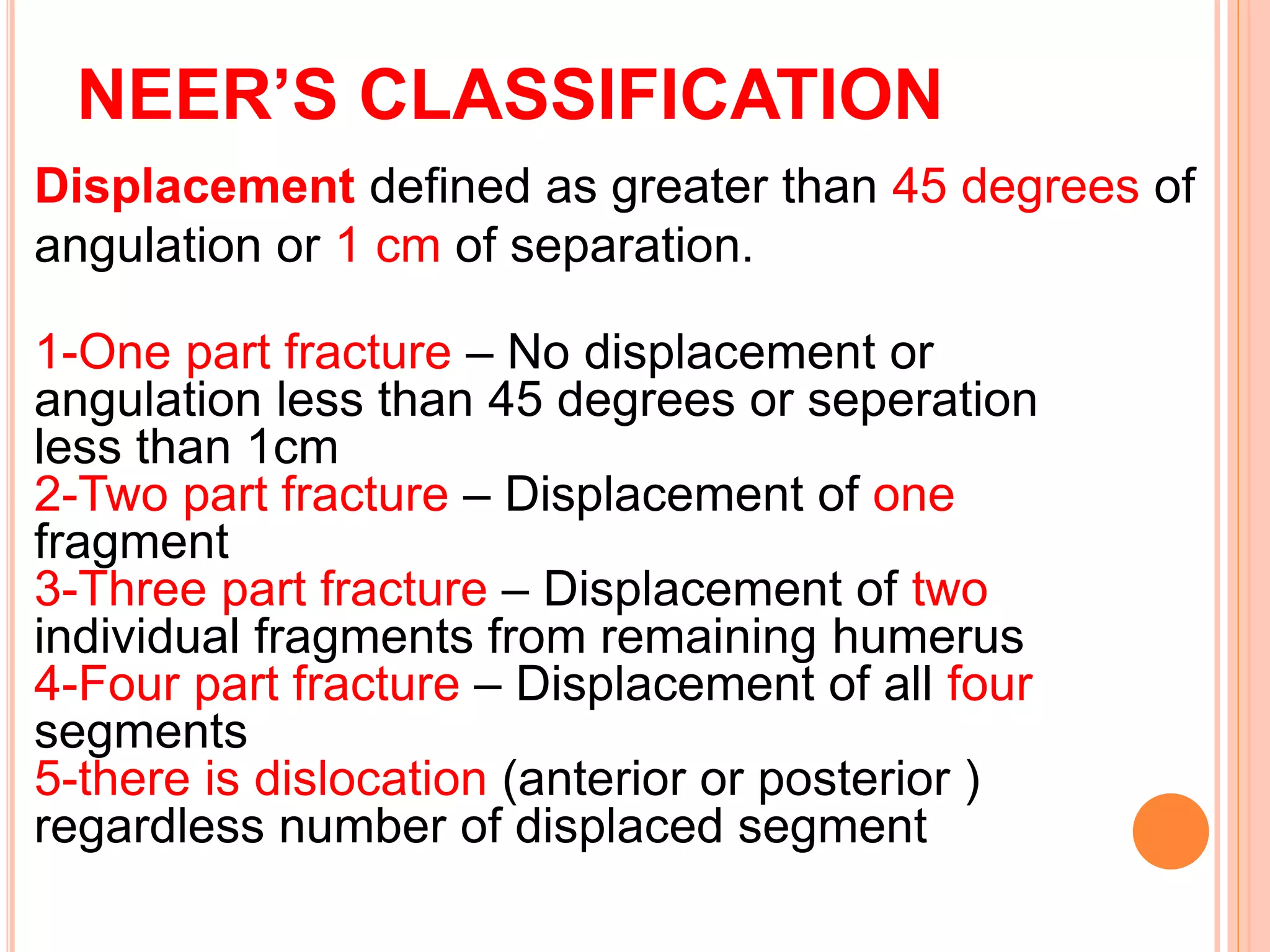
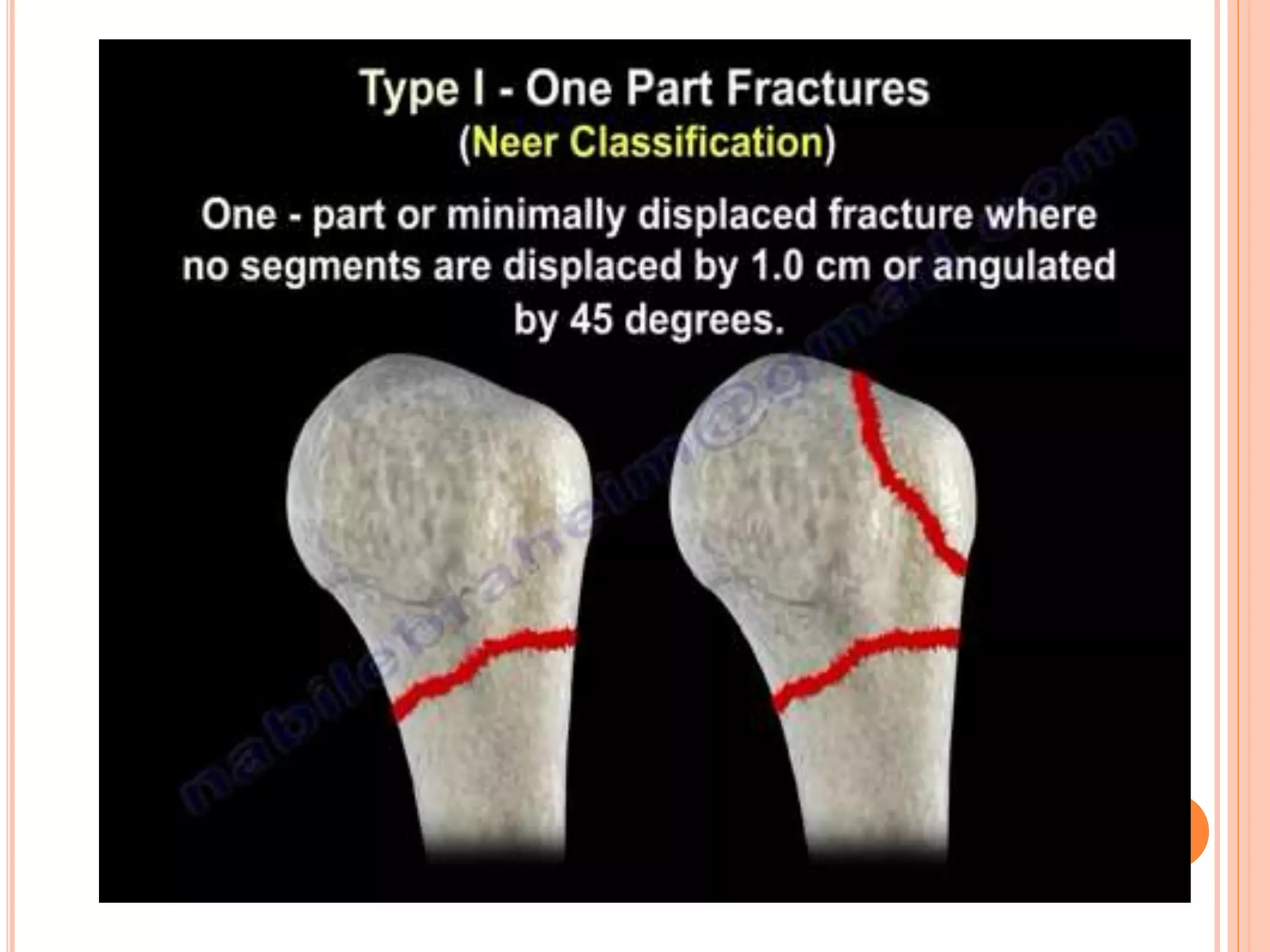
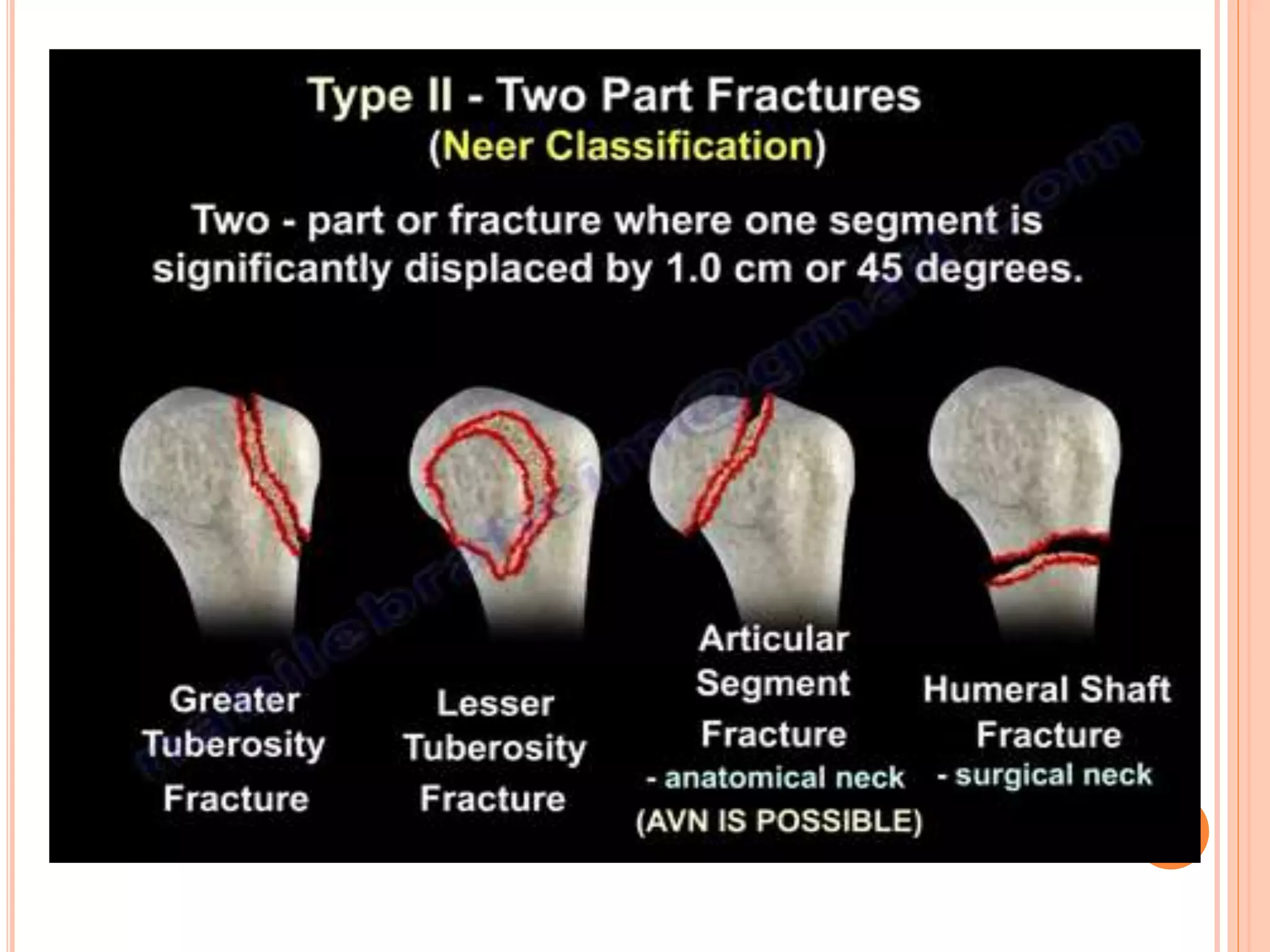
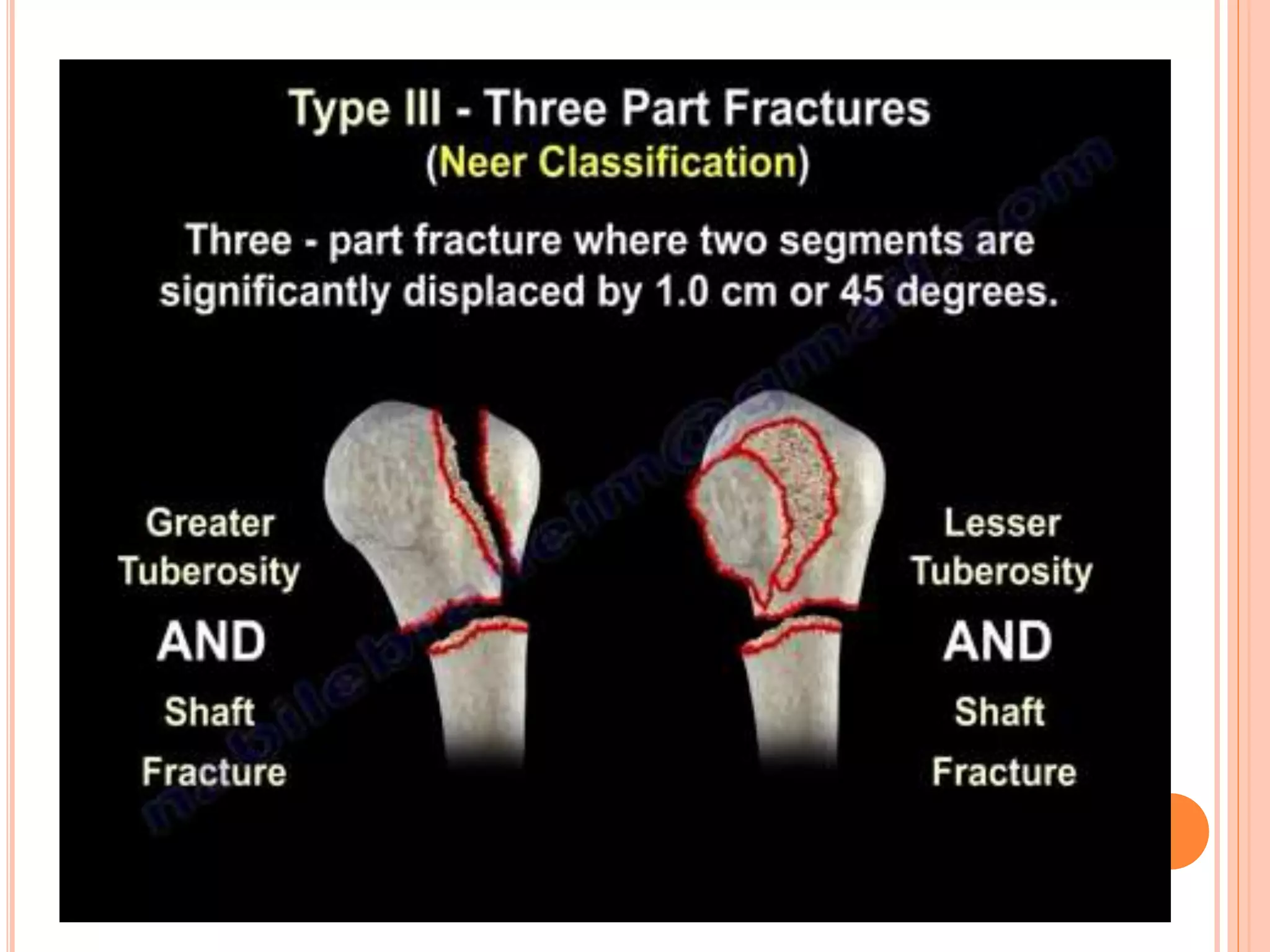
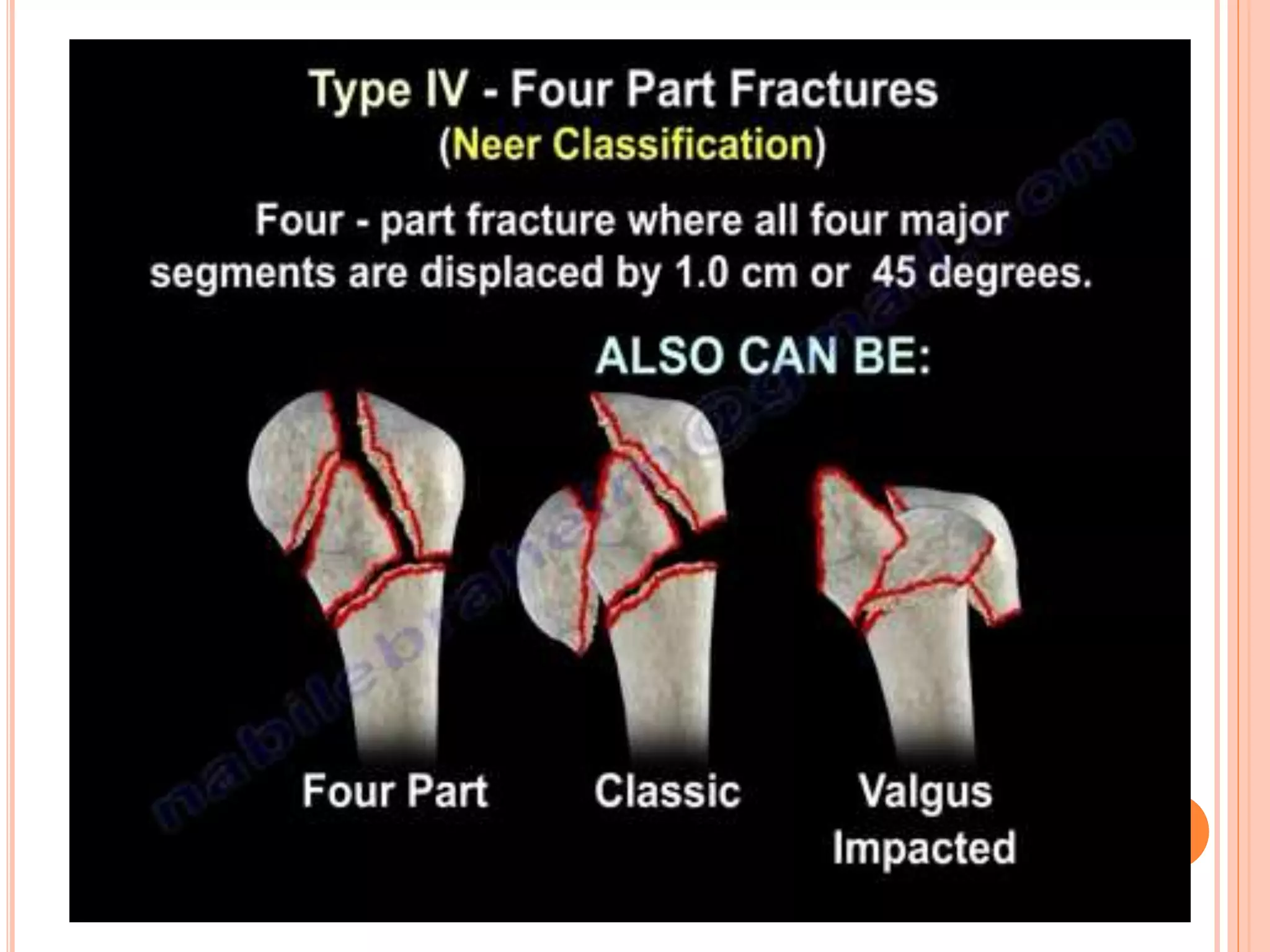
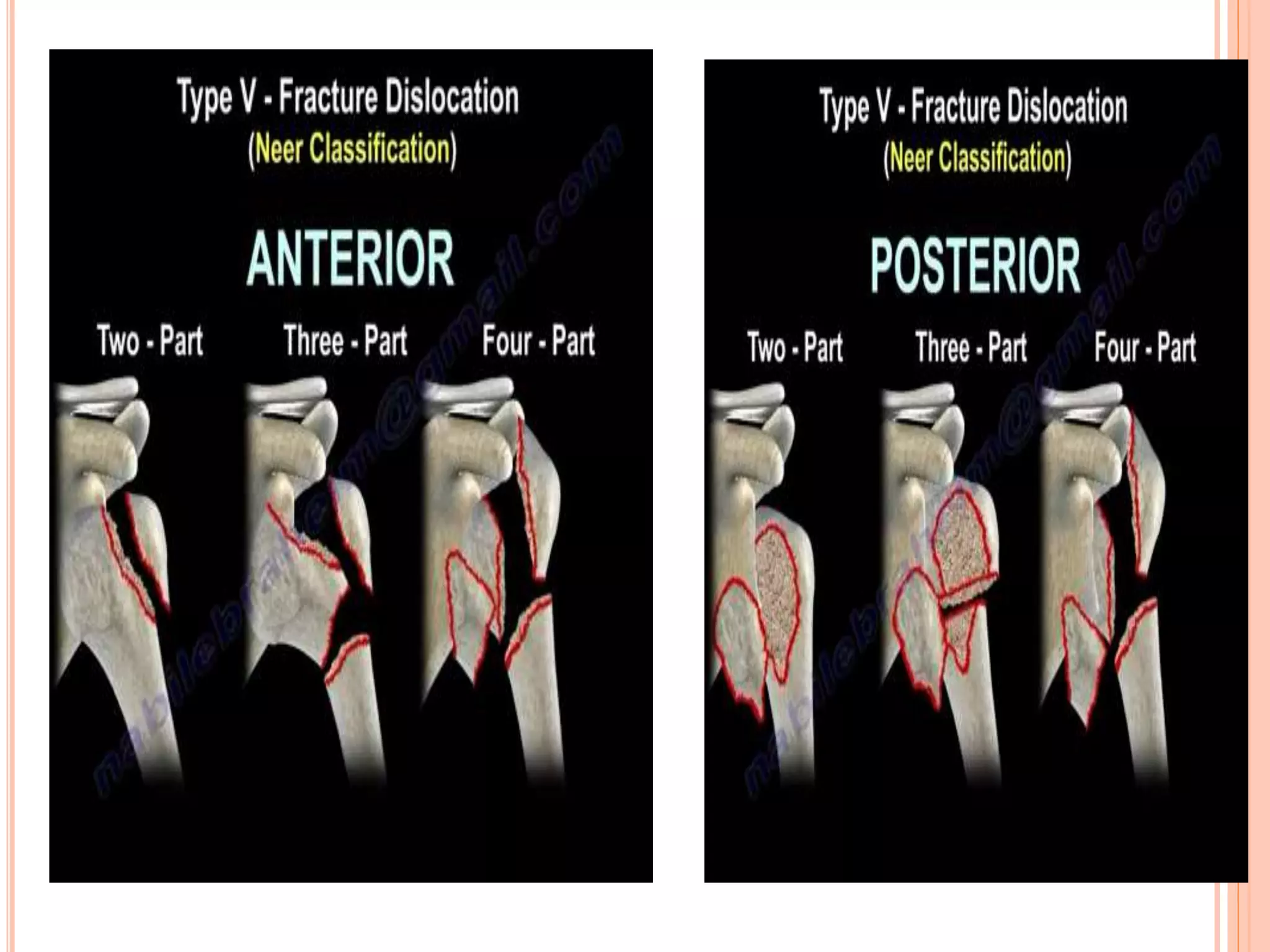


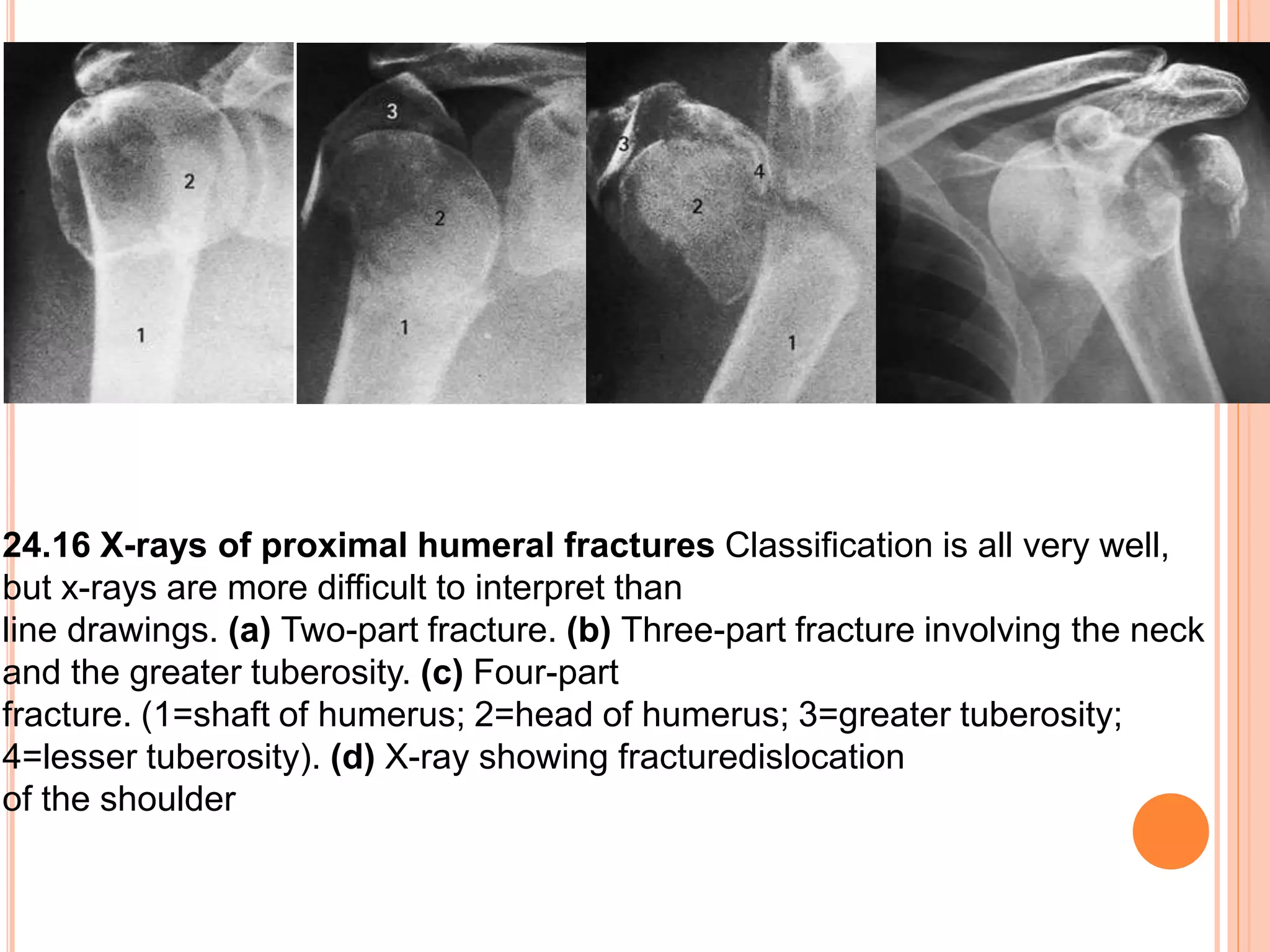

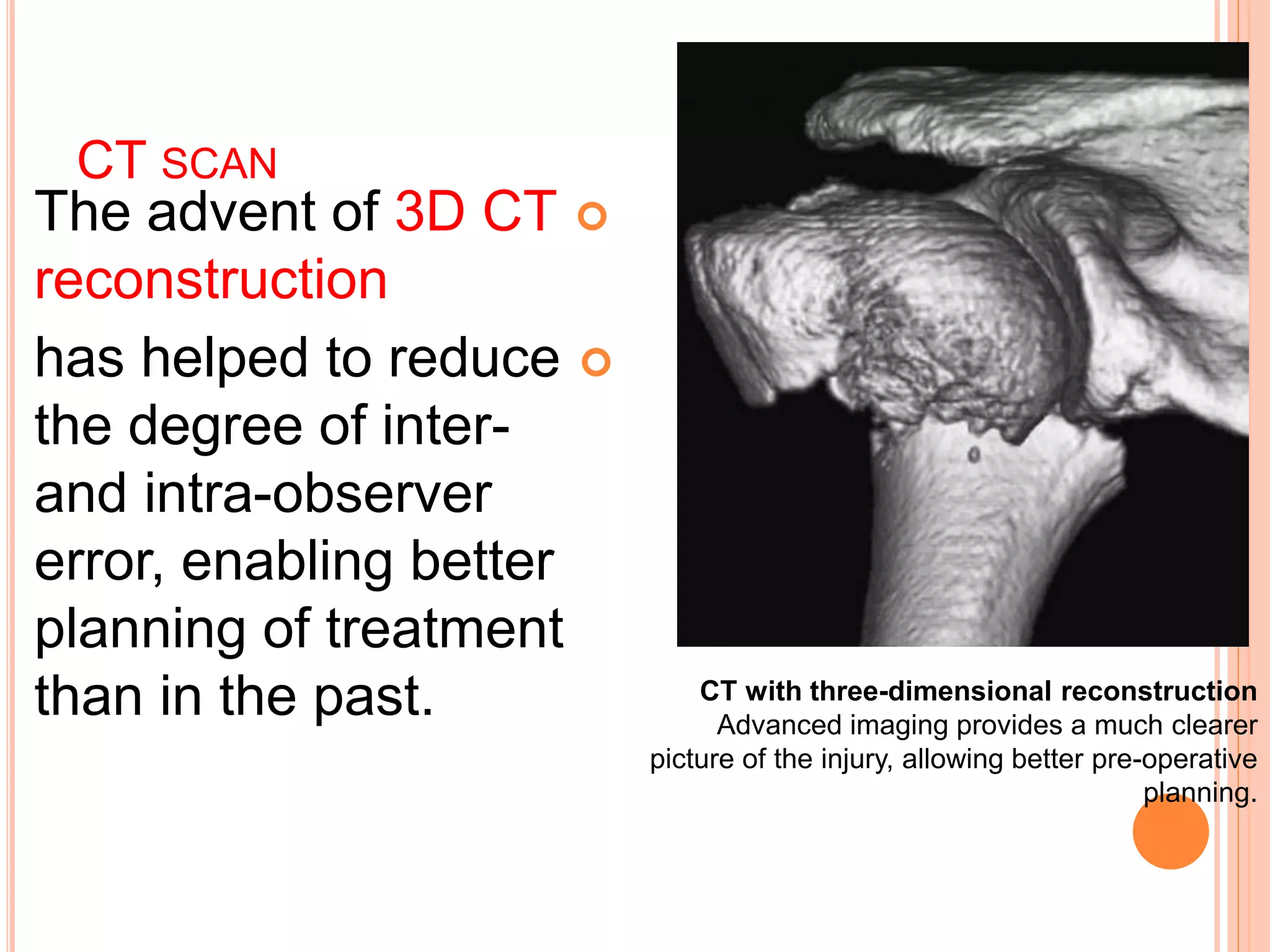


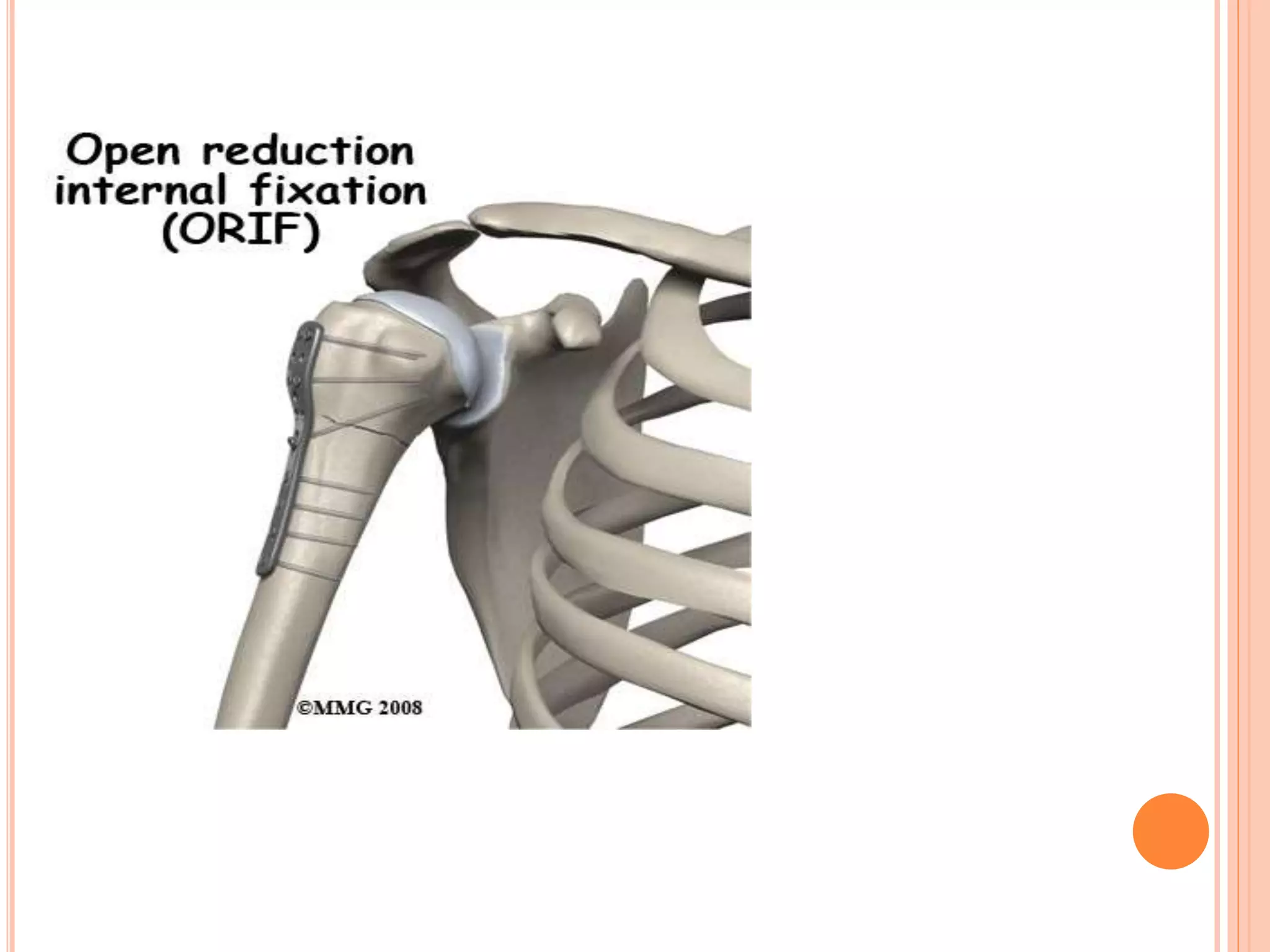


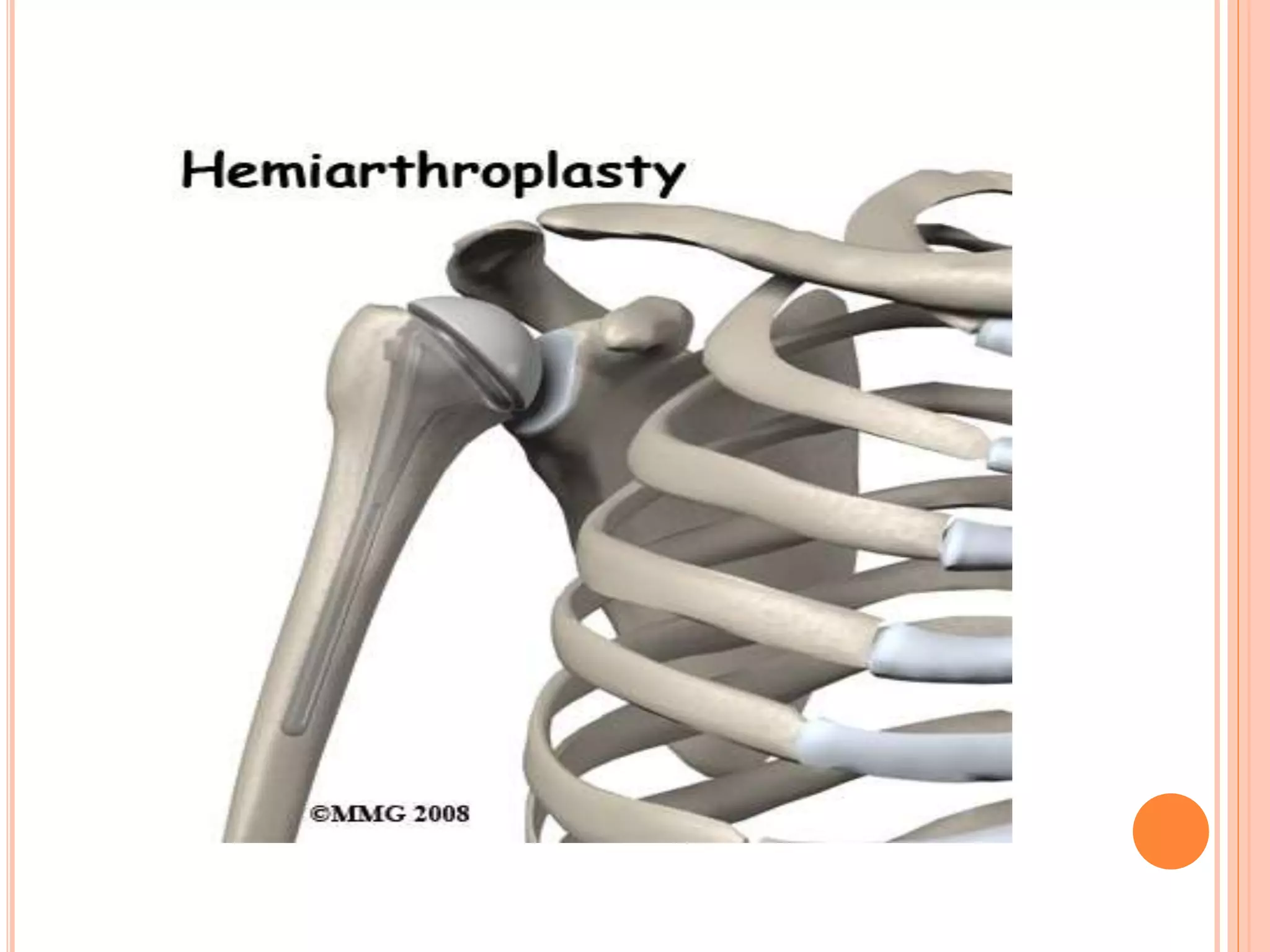



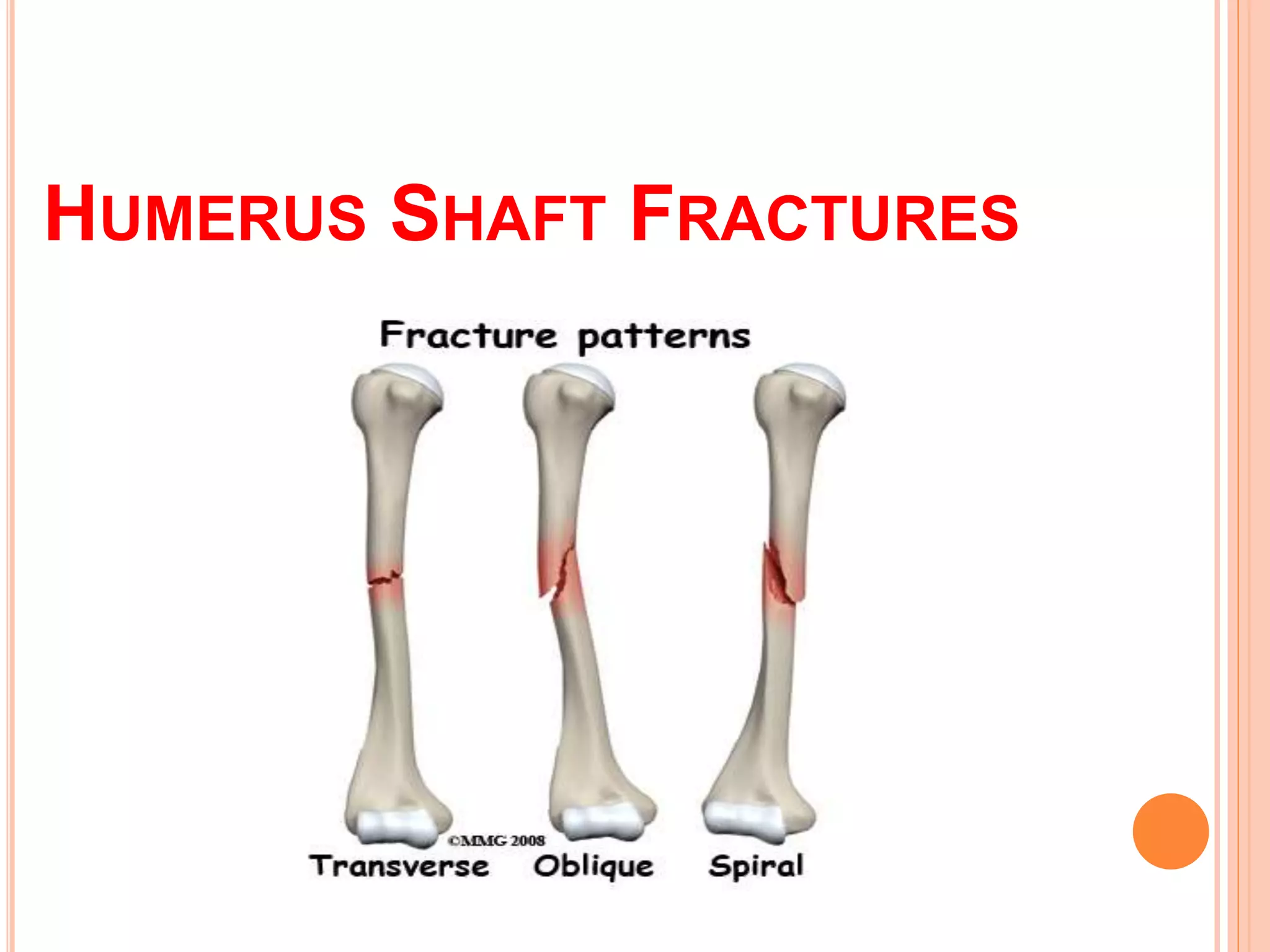
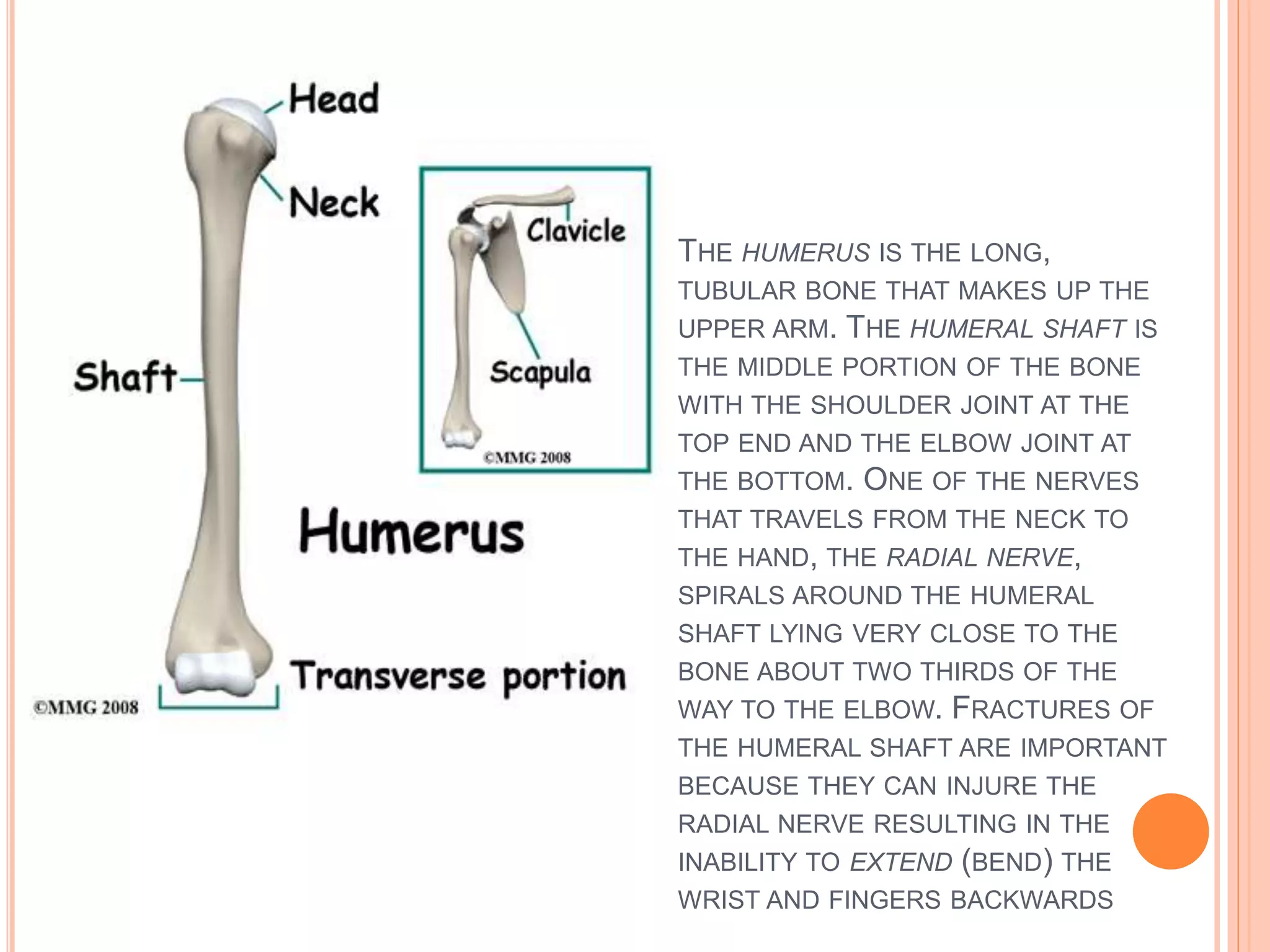
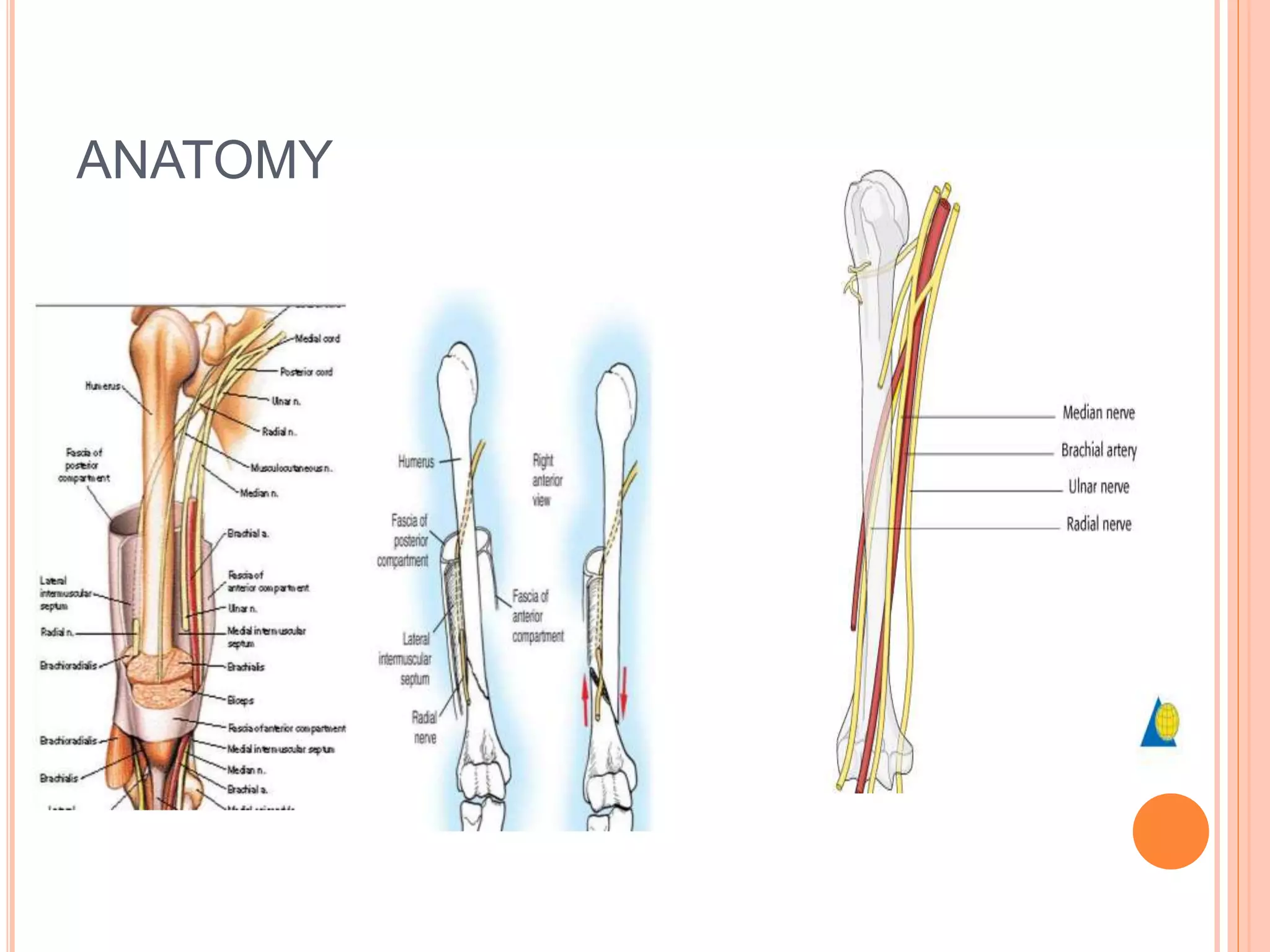

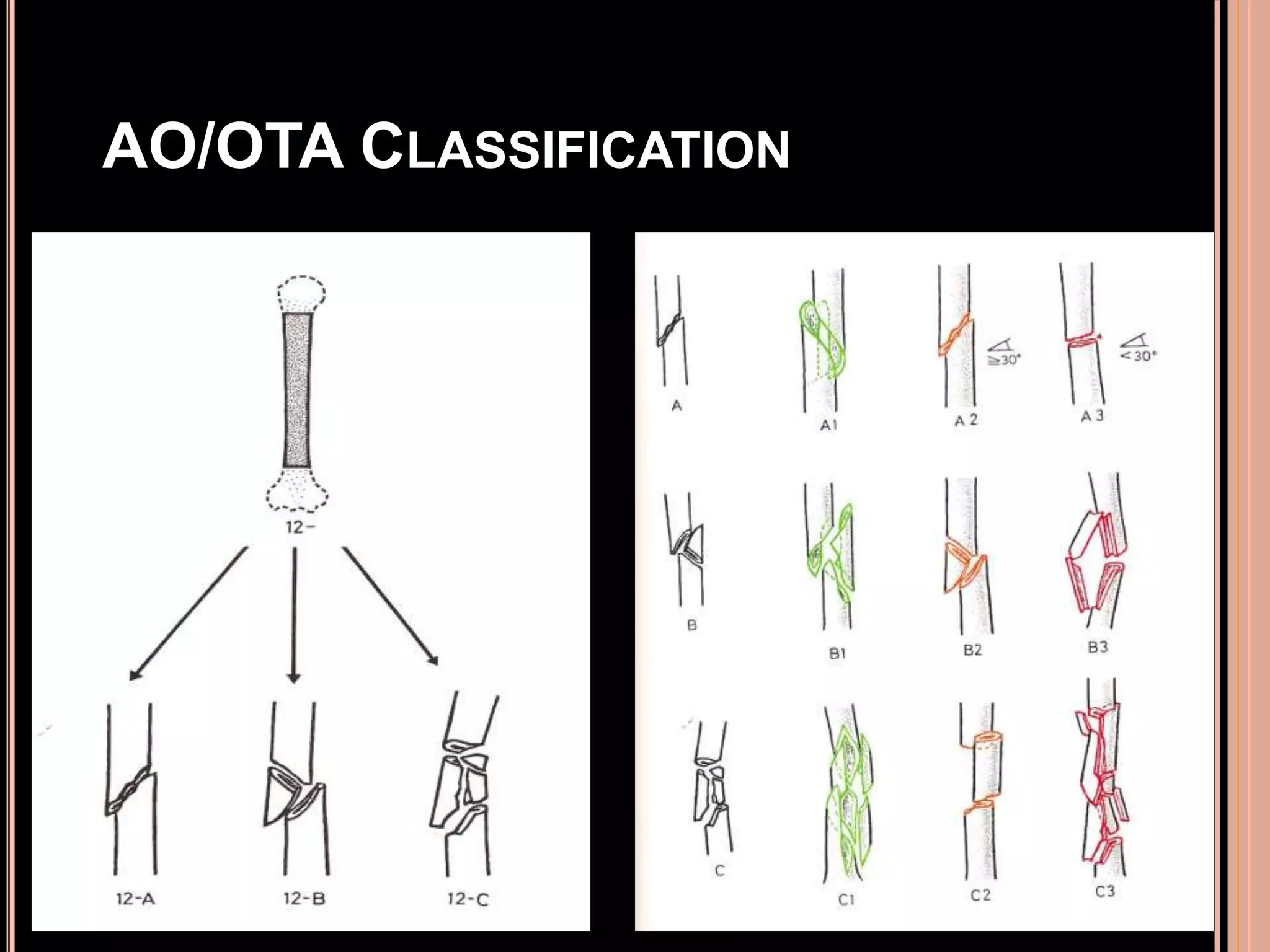




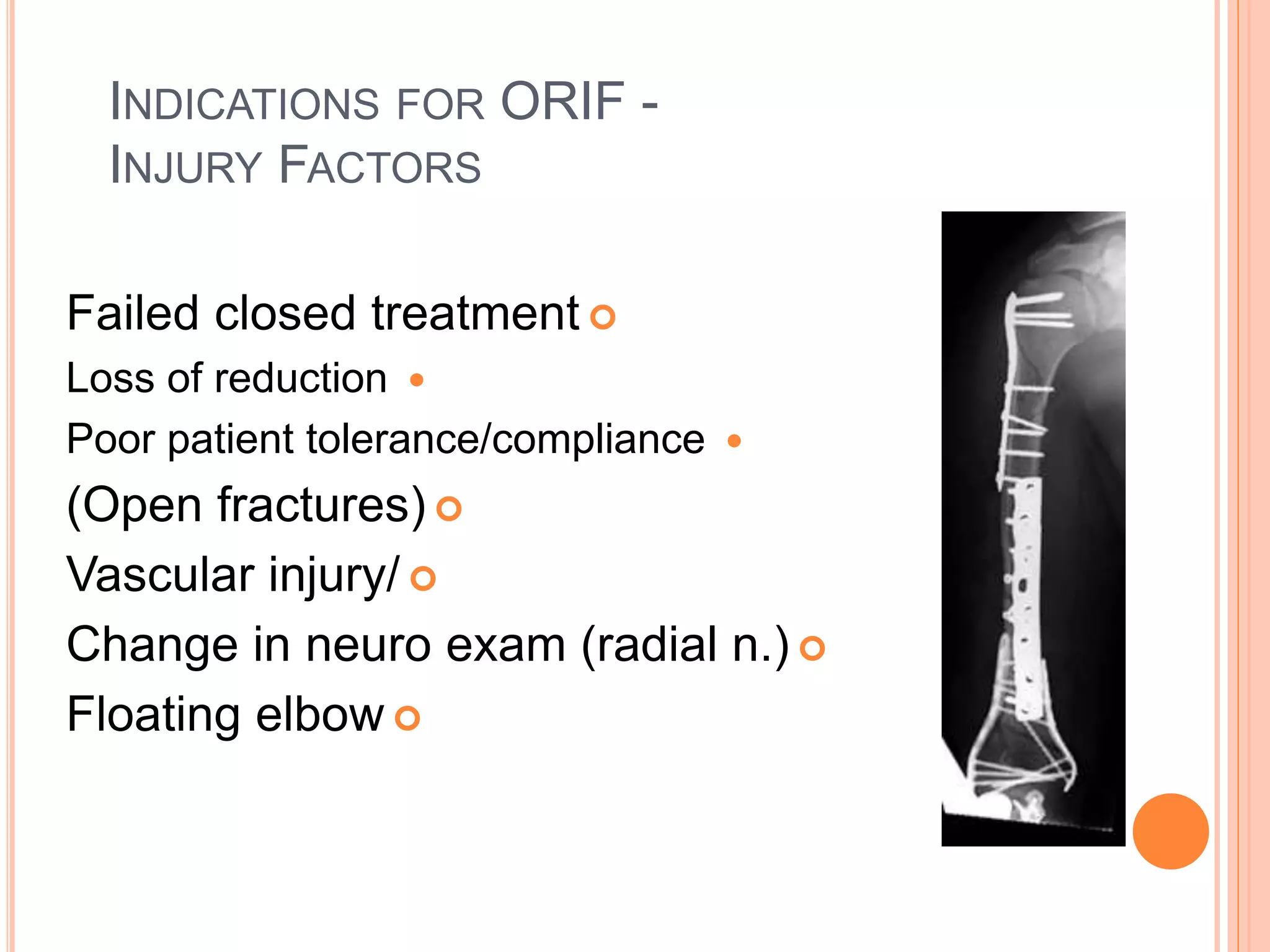











The document provides an overview of proximal humeral fractures, detailing their anatomy, classification systems, clinical presentation, diagnosis, and treatment options. Various classification systems, such as Neer's, Koucher's, and Codman's, are described to categorize the fractures based on displacement and anatomical features, with emphasis on the role of imaging in diagnosis. Treatment approaches vary based on the fracture type, with conservative management for one-part fractures, whereas more complex fractures may require surgical intervention due to complications like nerve injury or instability.











































































































