Downloaded 641 times
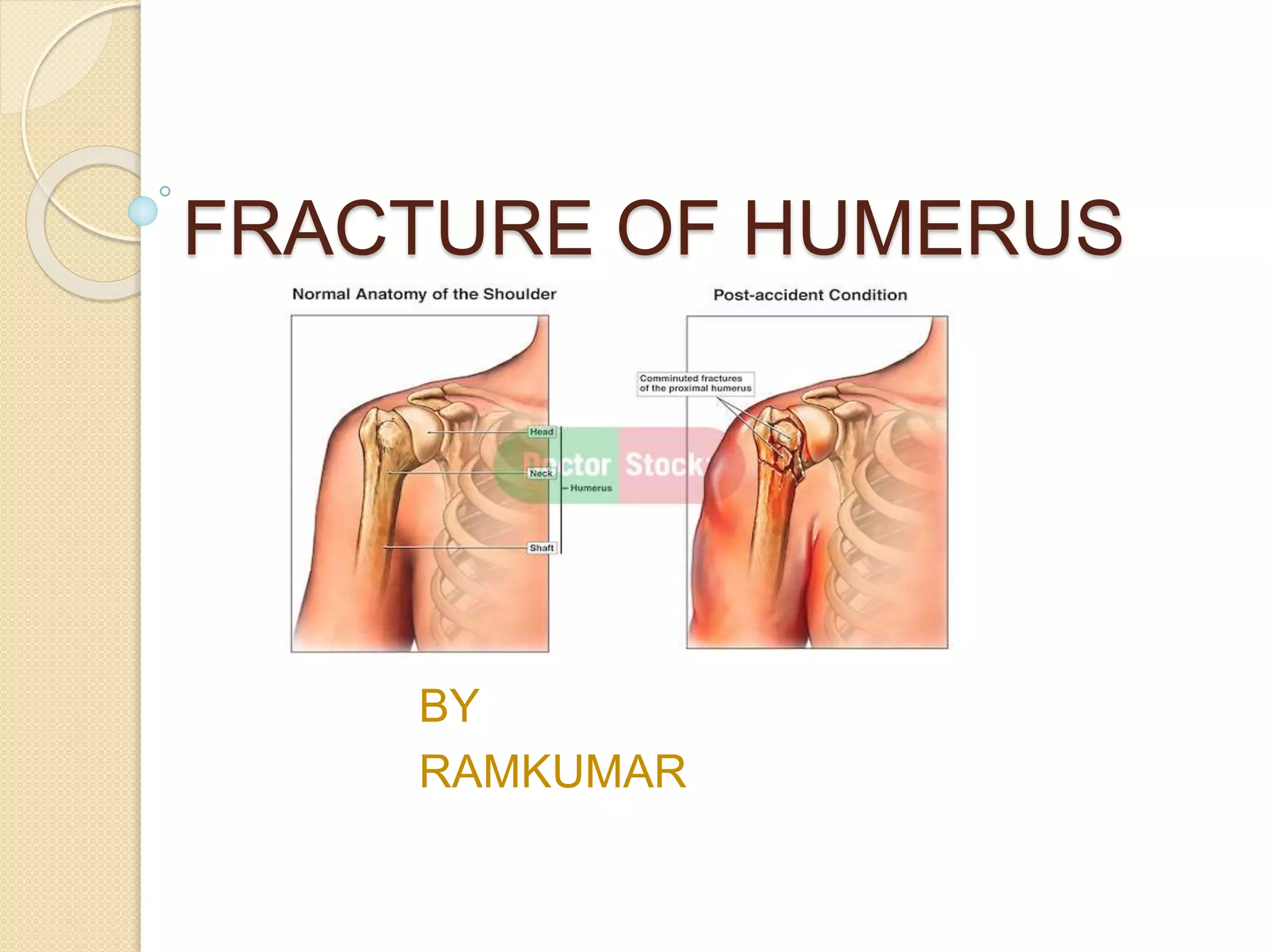
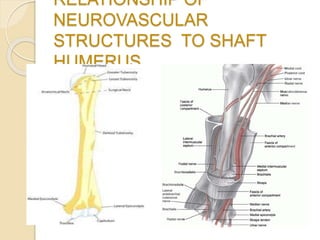

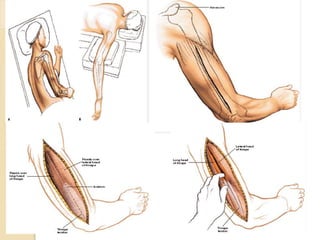

The document discusses fractures of the humerus bone in the upper arm. It describes the anatomy of the humerus and common mechanisms of injury including direct trauma and falls. Symptoms include pain, deformity, and abnormal mobility. Treatment involves splinting or casting for minor fractures and surgical intervention using plates, nails, or external fixation for more complex fractures. Complications can include nerve injuries, nonunion, malunion, and stiffness.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

