Downloaded 807 times


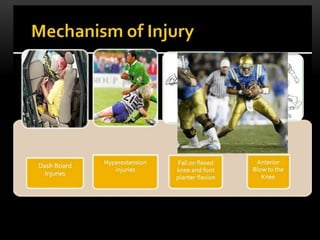









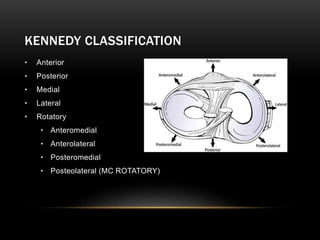

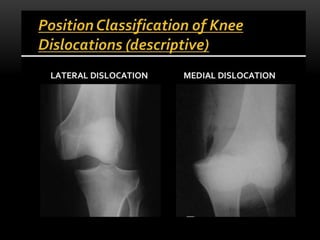
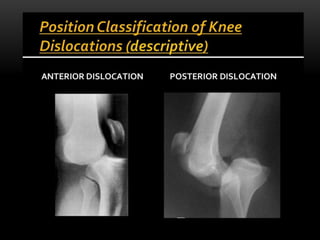




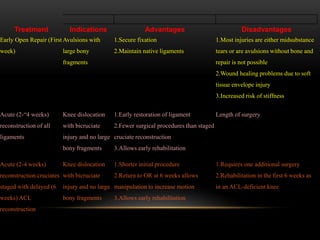


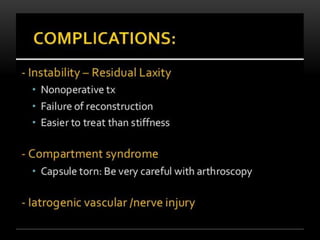


This document discusses knee dislocations, including their epidemiology, stabilizers of the knee joint, clinical features, associated injuries, imaging, and classifications. It also reviews treatment indications and options for knee dislocations, such as early open repair, acute reconstruction, staged reconstruction, and use of an external fixator. Complications include stiffness, which can be addressed through early range of motion exercises and manipulation if needed.



































































