Presentation1, radiological imaging of corpus callosum lesios.
•Download as PPTX, PDF•
12 likes•2,790 views

1. The corpus callosum is commonly involved by lesions from various etiologies including congenital abnormalities, demyelination, infection, leukodystrophy, neoplasms, trauma, and vascular causes. 2. Transient lesions of the splenium are often seen in association with epilepsy, antiepileptic drug changes, infections, electrolyte imbalances, and PRES. They typically appear hyperintense on T2/FLAIR and DWI with restricted diffusion resolving within 1 month. 3. Common neoplasms involving the corpus callosum include glioblastoma, which may appear as a "butterfly" lesion crossing the genu, and primary CNS lymphoma presenting with a similar pattern

More Related Content
What's hot
What's hot (20)
Similar to Presentation1, radiological imaging of corpus callosum lesios.
Similar to Presentation1, radiological imaging of corpus callosum lesios. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological imaging of corpus callosum lesios.
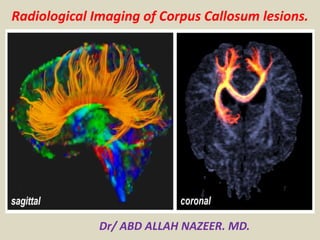
- 1. Radiological Imaging of Corpus Callosum lesions. Dr/ ABD ALLAH NAZEER. MD.
- 2. Normal anatomy of the corpus callosum. T1-weighted (left), T2-weighted (middle), and FLAIR (right) MR images show the corpus callosum (CC). The splenium is the most posterior and thickest portion of the CC.
- 3. Lesions of the corpus callosum are uncommon and arise from multiple different etiologies. The lesions can be classified according to underlying Pathophysiology . Congenital agenesis of the corpus callosum enlarged perivascular spaces tubonodular pericallosal lipoma: associated with dysgenesis of the corpus callosum. Demyelination acute disseminated encephalomyelitis Marchiafava-Bignami disease: demyelination and necrosis, can appear as cystic lesions multiple sclerosis neuromyelitis optica progressive multifocal leukoencephalopathy Susac syndrome wallerian degeneratio
- 4. Infection aspergillosis: can involve corpus callosum transient lesions of the splenium: many underlying etiologies including infectious agents subacute sclerosing panencephalitis: can involve the corpus callosum in advanced stages tuberculosis: callosal tuberculomas have been reported, although rare Leukodystrophy Krabbe disease metachromatic leukodystrophy Susac syndrome X-Linked adrenoleukodystrophy Neoplasm Typically, amongst neoplasms, only aggressive lesions can invade the corpus callosum as it is composed of very dense white matter tracts which act as a barrier to tumour spreading. anaplastic astrocytoma callosal oligodendroglioma glioblastoma (butterfly glioma) gliomatosis cerebri meningioma: secondary involvement from primary falx lesion metastasis: rare, mainly from contiguous extension of lesion adjacent to corpus callosum primary CNS lymphoma
- 5. Other corpus callosum impingement syndrome transient lesion of the splenium: many underlying aetiologies post shunt decompression: after placement of ventriculostomy in patients with chronic hydrocephalus Trauma diffuse axonal injury Vascular aneurysm: can occasionally rupture into the corpus callosum arteriovenous malformation: arising around the corpus callosum cavernous malformation (cavernoma) gliosis: secondary to small vessel chronic ischemia, subcortical arteriosclerotic encephalopathy and radiation therapy; histologically corresponds to subependymal gliosis hypoxic-ischemic encephalopathy: corpus callosum only involved in severe or advanced case infarction: rare because of extensive collateral vascular supply, most often seen with emboli, major ischaemic stroke, subfalcine herniation with mass effect and vasculitides.
- 6. Transient lesions of the splenium of the corpus callosum, also known as mild encephalitis/encephalopathy with a reversible isolated SCC lesion (MERS), are occasionally encountered on MRI studies and may be due to a number of underlying etiologies. Clinical presentation Unlike other causes of splenium of corpus callosum (SCC) lesions, the small transient lesions of the splenium seen in epilepsy and antiepileptic drug cessation use do not demonstrate convincing signs or symptoms of hemispheric disconnection, such as pseudo-neglect, alien hand syndrome, apraxia of the left hand, agraphia, alexia, and visual apraxias.
- 7. Aetiology epilepsy classic presentation is seen in patients with sudden cessation of antiepileptic drugs seizures: focal lesions have been described after focal status epilepticus and unusually after single seizures and were explained as focal brain edema. electrolyte imbalance including extrapontine myelinolysis demyelination multiple sclerosis (MS) acute disseminated encephalomyelitis (ADEM) posterior reversible encephalopathy syndrome (PRES) Marchiafava-Bignami disease diffuse axonal injury (DAI) AIDS dementia complex infections viral: influenza, measles, herpes, mumps, adenovirus, varicella zoster, rotavirus and HIV bacterial: salmonella, Legionnaires' disease mycobacterial: tuberculous meningitis hypoglycemia hemolytic-uremic syndrome with encephalopathy.
- 8. Radiographic features Transient lesions of the splenium are only really appreciable on MRI where they have two distinct patterns: well circumscribed, small, oval lesions in the midline within the substance of the corpus callosum more extensive ill-defined irregular lesions extending throughout the splenium and into the adjacent hemispheres (boomerang sign) The smaller well-circumscribed lesions are the typical lesion seen in the setting of seizures/cessation of antiepileptic medication, whereas the larger lesion is more typical of other etiologies. MRI These lesions tend to demonstrate the following signal characteristics: T1: hypointense T2: hyperintense DWI/ADC: restricted diffusion T1 C+: no enhancement Studies have shown that patients recover completely on MRI studies within 1 month, mostly within 1 week following the neurologic recovery .
- 9. A 1-year-old female patient with complete corpus callosal agenesis. T1-weigted axial image (left) shows parallel configuration of both lateral ventricles. T1-weighted sagittal image (right) reveals complete agenesis of the corpus callosum.
- 10. Agenesis of corpus callosum. A, Sagittal midline T1-weighted image shows complete absence of corpus callosum (arrows). Axial T2-weighted image shows colpocephalic configuration with dilated occipital horns, right greater than left (asterisks), and parallel (racecar) orientation of lateral ventricles. Third ventricle (arrow) is high riding and forms interhemispheric arachnoid cyst. Axial T2-weighted image at higher level illustrates crescentic (teardrop) morphology of frontal horns (arrows).
- 11. lipoma of corpus callosum. Coronal T1- weighted MR image shows large well-defined homogeneous midline mass lesion in region of corpus callosum with characteristic bright signal of lipoma. Note associated dysgenesis of corpus callosum. Corpus callosal Agenesis with Lipoma.
- 12. A 70-year-old male patient with a pericallosal lipoma and partial corpus callosal agenesis. Axial CT image (left) shows a lipoma in frontal interhemispheric fissure. There is a linear calcification at left side of the lesion. Sagittal T1-weighted MR image (right) reveals partial agenesis of the corpus callosum and a hyperintense pericallosal lipoma.
- 13. A 64-year-old male patient with a pericallosal lipoma and partial corpus callosal agenesis. T1-weighted axial (left) and sagittal (right) images show a hyperintense lipoma superior and posterior to the corpus callosum (CC). The CC shows partial agenesis. The splenial portion is not fully developed.
- 14. Callosal infarcts. A, Left anterior cerebral artery infarct (thick arrow) with extension into genu (thin arrow) is seen on diffusion-weighted (left) and apparent diffusion coefficient (ADC) (right) images, which confirm reduced diffusivity in these areas.
- 15. A 62-year-old male patient with acute splenial infarction. Axial FLAIR image (left) and DWI (middle) show multiple hyperintense lesions in bilateral basal ganglia, left thalamus, the splenium of the corpus callosum, and left occipital lobe. The lesions are more conspicuously demonstrated on DWI than on FLAIR image. ADC map image (right) reveals restricted water diffusion of the lesions.
- 16. A 70-year old female patient with chronic splenial infarction. Axial FLAIR (left) and sagittal T2-weighted (middle) images show a hyperintense lesion in the splenium of the corpus callosum. On DWI (right), the lesion is seen as isointensity.
- 17. Traumatic brain injury. A, Unenhanced CT images at level of lateral (A) and third (B) ventricles show hyperdense areas of acute hemorrhage in splenium (S) and genu (G). T2* gradient recalled-echo MR images at same levels confirm magnetic susceptibility in these areas. There are multiple additional foci of microhemorrhage throughout gray-white matter junction and basal ganglia (arrows).
- 18. 9-year-old female patient with Wallerian degeneration due to intracerebral hematomas. A, B. Axial T2 (A) and T1-weighted (B) images show two hyperintense hematomas in right occipital lobe (thick arrows) and left temporooccipital lobes (asterisks). There is moderate amount of surrounding brain edema. Splenium also shows mild swelling and increased signal intensity (thin arrows). C. Follow-up T2-weighted image obtained 20 months later reveals atrophic change and increased signal intensity of splenium (thin arrows).
- 19. A 29-year-old female patient with diffuse axonal injury lesion. She had a motor vehicle accident 9 days age. Axial FLAIR (left) and DWI (middle) images show a hyperintense lesion in the splenial portion of the corpus callosum. The lesion is more conspicuously demonstrated on DWI than on FLAIR image. ADC map image (right) reveals restricted water diffusion of the lesion.
- 20. A 29-year-old female patient with diffuse axonal injury lesion. Follow-up MR images were obtained 17 months later. On axial T2 (left), FLAIR (middle) and DWI (right) images, the splenial lesion has disappeared.
- 21. A 27-year-old male patient with diffuse axonal injury lesion. He had a motor vehicle accident 2 days age. Axial FLAIR (left) and DWI (middle) images show a focal hyperintense lesion in the splenial portion of the corpus callosum. The lesion is more conspicuously demonstrated on DWI than on FLAIR image. ADC map image (right) reveals restricted water diffusion of the lesion.
- 22. A 56-year-old male patient with diffuse axonal injury lesions. He had a motor vehicle accident 4 months age. Axial FLAIR image (left) shows a hyperintense lesion in the splenial portion of the corpus callosum. On DWI (middle), the lesion is seen as hypointensity. GE T2*-weighted image (right) reveals tiny hemorrhagic foci in the splenial lesion. There are also multiple tiny hemorrhage in right thalamus and left frontal white matter.
- 23. A 2-month-old female patient with hypoxic-ischemic encephalopathy. She had hypoxic insult 3 days ago. Axial DWI (left) shows diffuse hyperintense lesions in the bilateral cerebral cortices and white matter including the genu and splenium of the corpus callosum. ADC map image (right) reveals restricted water diffusion of the lesions
- 24. 2-month-old female patient with hypoxic-ischemic encephalopathy. Follow-up MR images were obtained 9 days later (12th day from hypoxic insult). On axial T2-weighted image (left) and DWI (middle left), the bilateral basal ganglia and thalami are newly involved and the corpus callosal (CC) lesions show more prominent hyperintensities compared to on initial DWI. Both cerebral cortices and white matter lesions are decreased in their signal intensities. ADC map image (middle right) reveals restricted water diffusion of the CC lesions. On contrast-enhanced T1-weighted image, there is strong contrast enhancement along the cortices and subcortical white matter of both cerebral hemispheres.
- 25. 2-day-old female with hypoglycemic encephalopathy. Glucose level was 2 mg/dL at presentation. A. On FLAIR axial image, there is no definite lesion. B. Axial DWI shows hyperintense lesions in both occipital lobes and splenium (arrows). C. ADC map image reveals restricted water diffusion of lesions (arrows). ADC = apparent diffusion coefficient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
- 26. 8-year-old female patient with CO-intoxication. Axial FLAIR image (A) and DWI (B) show multiple hyperintense lesions in bilateral globus pallidus (arrowheads) and cerebral white matter (thin arrows) including splenium of corpus callosum (thick arrows). DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
- 27. 59-year-old male patient with chronic alcoholism. A, B. FLAIR (A) and T2-weighted (B) images show hyperintense lesions in body (thin arrows) and splenial portion (thick arrows) of corpus callosum. C. There is focal contrast enhancement of lesions (arrows) on post-contrast T1-weighted image. FLAIR = fluid-attenuated inversion recovery
- 28. 5-day-old male with rotavirus-related white matter injury. A, B. Initial axial DWI (A) and ADC map (B) demonstrate extensive areas of restricted diffusion in periventricular white matter, deep white matter, corpus callosum, internal capsule, and posterior thalami. C. Follow-up FLAIR image obtained five years later shows residual ischemic lesions due to previous white matter injury in both periventricular white matters (arrows). ADC = apparent diffusion coefficient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
- 29. Multiple sclerosis who presented with visual complaints. Sagittal MR image shows multiple hyperintense lesions (arrows) in corpus callosum.
- 30. Axial brain MRI (fluid-attenuated inversion recovery) with tumefactive lesions (A) developed exacerbation 67 days after the start of interferon-β-1b (IFNβ-1b) therapy; MRI showed huge tumefactive lesion in right hemisphere. Case 5 (B) developed exacerbation 32 days after the start of IFNβ-1b therapy; MRI showed tumefactive lesions in corpus callosum extending to the right parietal white matter.
- 31. 4-year-old girl with pilocytic astrocytoma. Axial T2- weighted MR image shows that lesion is hyperintense. 4-year-old girl with pilocytic astrocytoma. Sagittal T1- weighted MR image shows well-circumscribed hypointense lesion in body of corpus callosum. 4-year-old girl with pilocytic astrocytoma. Enhanced coronal T1- weighted MR image shows marked contrast enhancement of lesion.
- 32. A 59-year-old female patient with a glioblastoma. Axial T2-weighted image (left) and DWI (middle left) show a large heterointense mass in right temporoparietal white matter and adjacent splenium of the corpus callosum. There is large amount of surrounding brain edema. Perfusion MR image (middle right) reveals increased perfusion in the peripheral solid portion of the mass. On contrast- enhanced T1-weighted image, there is peripheral rim enhancement of the mass.
- 33. Glioblastoma multiforme. A, Unenhanced CT image shows heterogeneously hypodense mass with surrounding vasogenic edema. This involves both frontal lobes and crosses genu (G) of corpus callosum, producing butterfly appearance. There is compression and distortion of frontal horns of both lateral ventricles. Contrast-enhanced T1-weighted MR image shows involvement of genu (G). Lesion shows rim enhancement and central hypointensity, compatible with necrosis.
- 34. A 46-year-old female patient with gliomatosis cerebri. Axial FLAIR image (left) show an ill-defined hyperintense lesion involving bilateral posterior cerebral white matter and the splenium of the corpus callosum. On enhanced T1-weighted axial image (middle), there is no definite contrast enhancement of the lesion. Single voxel 1H MR spectroscopy (right) reveals increased choline peak.
- 35. Nonimmunocompromised woman with primary central nervous system lymphoma who presented with disorientation. MRI show lesion (arrow) of left parieto— occipital white matter, crossing corpus callosum in classic butterfly pattern.
- 37. A 23-year-old male patient with a pineal germinoma. Axial T2 (left) and T1- weighted (middle) images show a mass in the pineal area. The mass extends into the 3rd ventricle anteriorly and to the splenium of the corpus callosum posteriorly. On enhanced T1-weighted image, the mass is strongly enhanced.
- 38. A 62-year-old male patient with epilepsy. Axial DWI (left) shows a focal hyperintense lesion in the splenium of the corpus callosum. ADC map image (middle) reveals restricted water diffusion of the lesion. On follow- up DWI (right) obtained 14 days later, the splenial lesion has disappeared.
- 39. A 38-year-old female patient with bacterial meningoencephalitis due to S. pneumoniae. Axial FLAIR image (left) and DWI (middle) show a hyperintense lesion in the splenium of the corpus callosum. The lesion is more conspicuously demonstrated on DWI than on FLAIR image. There is tissue loss in left frontal lobe. ADC map image (right) reveals markedly restricted water diffusion of the splenial lesion.
- 40. A 15-year-old male patient with abc meningoencephalitis. Axial FLAIR image (left) and DWI (middle) shows a focal hyperintense lesion in midline corpus callosum. The lesion is more conspicuously demonstrated on DWI than on FLAIR image. ADC map image (right) reveals markedly restricted water diffusion of the lesion.
- 41. Transient splenial intensity changes. A, Example images in migraine and visual scotomas (A), adenovirus encephalitis (B), and metronidazole toxicity (C) show FLAIR hyperintensity and reduced diffusivity in splenium (arrows), which resolved on follow-up imaging.
- 42. A 59-year old male patient with chronic alcoholics. FLAIR (left) and T2-weighted (middle) images show hyperintense lesions in the body and splenial portion of the CC. There is focal contrast enhancement of the lesions on post-contrast T1-weighted image (right).
- 43. 2-year-old man with arteriovenous malformation who presented with intraventricular hemorrhage. Sagittal T1- weighted MR image shows hemorrhage (arrows) and multiple flow voids in corpus callosum. 2-year-old man with arteriovenous malformation who presented with intraventricular hemorrhage. Axial T2- weighted MR image shows hyperintense lesion (arrow) with flow voids.
- 44. Unenhanced CT and Gradient MR image in different patient who had ruptured anterior communicating artery aneurysm. Right pericallosal artery aneurysm (arrow). Aneurysm.
- 45. Unenhanced CT image shows round well- circumscribed hyperdense mass (asterisk) centered in falx cerebri (arrow) and extending across midline. There is subtle surrounding edema that involves bilateral temporo-occipital regions T1-weighted contrast-enhanced MR image shows relatively homogeneous contrast enhancement within mass, which deviates surrounding pial vessels (arrows).
- 46. Contrast-enhanced CT (A) and contrast- enhanced T1-weighted MR (B) images show heterogeneously enhancing dominant metastasis in left frontal lobe (asterisk). Additional enhancing foci are noted in splenium (S), genu (G), and periventricular regions (arrows). Contrast-enhanced CT (A) and contrast-enhanced T1-weighted MR (B) images show heterogeneously enhancing dominant metastasis in left frontal lobe (asterisk). Additional enhancing foci are noted in splenium (S), genu (G), and periventricular regions (arrows).
- 47. Hereditary leukoencephalopathies. A, FLAIR MR images show signal abnormalities in bilateral parietal lobes and intervening splenium of corpus callosum (arrows): metachromatic leukodystrophy (A) and adrenoleukodystrophy (B)
- 48. Periventricular leukomalacia. A, T2-weighted MR image shows periventricular white matter abnormalities, with increased signal in both frontal and parietal lobes as well as genu (G) and splenium (S) of corpus callosum. Susceptibility artifact within choroid plexus of occipital horns (asterisks) confirms presence of hemorrhage. Diffusion-weighted MR image identifies reduced diffusivity within splenium (arrows) and multiple other areas.
- 49. Virchow-Robin spaces in Hunter syndrome (mucopolysaccharidosis type 2). Axial FLAIR image shows diffusely enlarged perivascular spaces, which are isointense to CSF and involve body of corpus callosum (arrows). Sagittal T1 FLAIR contrast-enhanced image shows large Virchow-Robin spaces within corpus callosum (arrow) and brain parenchyma.
- 50. Marchiafava-Bignami disease. (Courtesy of Ginat DT, Massachusetts General Hospital, Boston, MA)A, FLAIR MR image shows increased signal in splenium (arrow). Marchiafava-Bignami disease. (Courtesy of Ginat DT, Massachusetts General Hospital, Boston, MA)B, Apparent diffusion coefficient map confirms reduced diffusivity in this region (arrow).
- 51. Susac's syndrome:(a-d) Magnetic resonance imaging FLAIR T2 image showing multiple well-defined hyperintense lesions in periventricular and callosal area. Magnetic resonance imaging T1 image showing hypointense lesions in center of corpus callosum. Magnetic resonance imaging, 4 weeks later showing almost complete disappearance of lesions
- 53. Magnetic resonance imaging of the brain: Diffusion-weighted sequences during 2010 episode (a-d) showing restricting lesions in left posterior limb of internal capsule and splenium of the corpus callosum. Lesions involving bilateral subcortical white matter and centrum semi ovale (e-h) during July 2013 episode. Resolution of the changes (i-l) in the repeat imaging done after 1.5 months. Arrows showing abnormalities.
- 54. Callosal thickening of neurofibromatosis type 1. A midsagittal T1W MR image shows diffuse thickening of the corpus callosum (arrows).
- 55. Thank You.