Downloaded 536 times
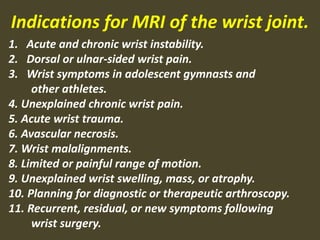
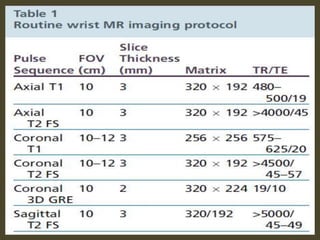
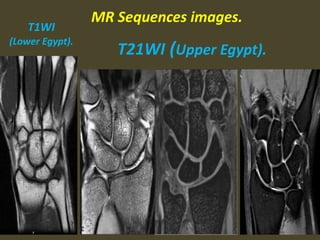
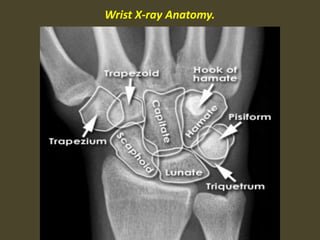

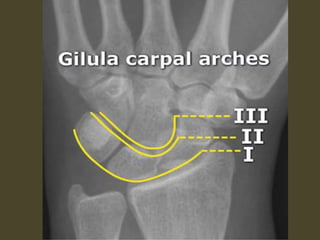
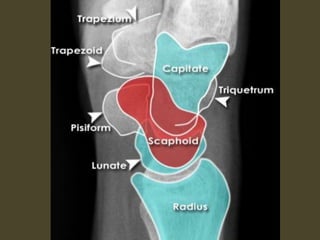

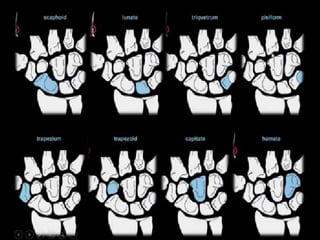
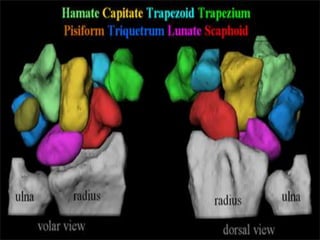

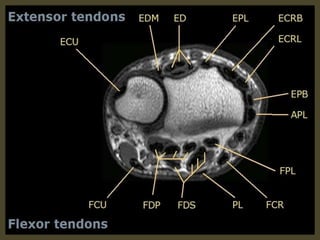
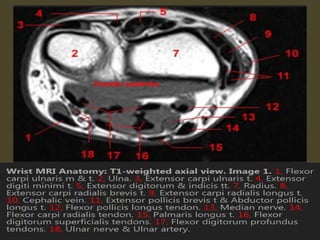
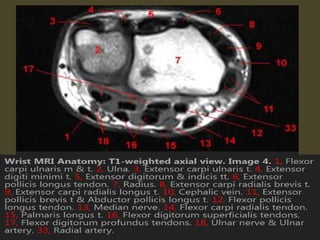
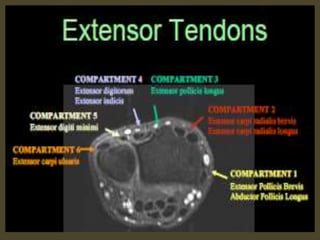
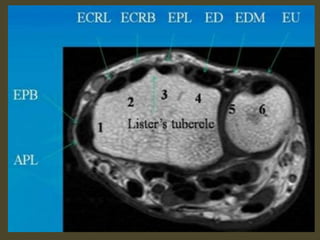
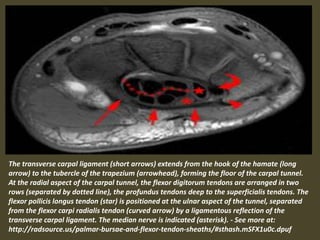
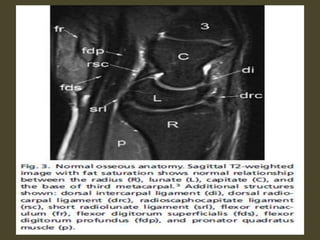
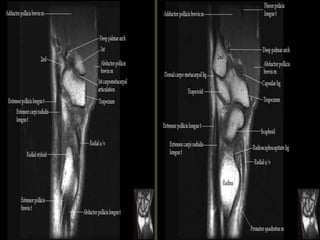
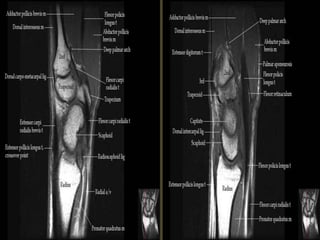

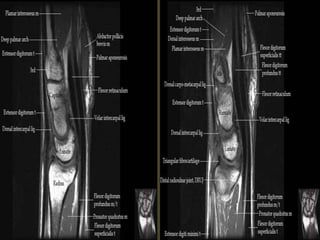
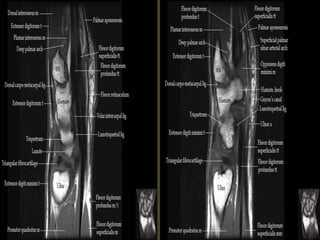
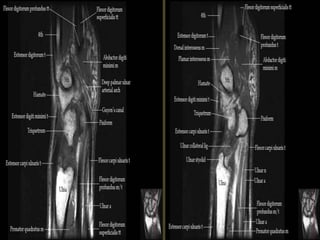

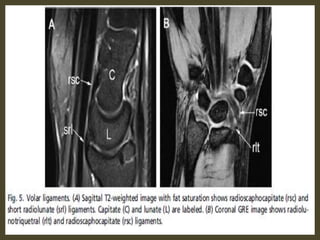
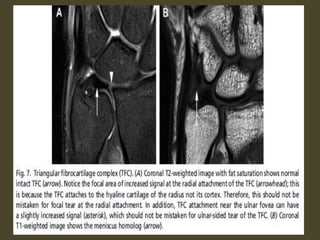


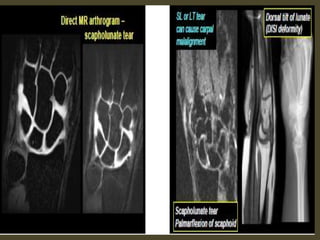

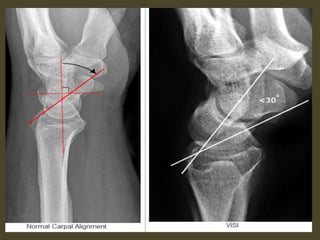

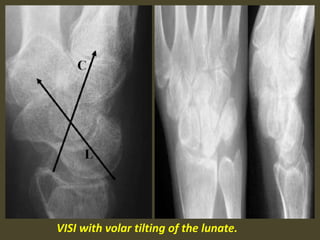












This document provides an overview of MRI indications and findings for wrist pathology. It lists common indications for MRI such as wrist instability, pain, trauma, necrosis, and limited range of motion. It then reviews MRI sequences, wrist anatomy, and various wrist conditions that may be seen on MRI such as fractures, ligament tears, instability patterns, tenosynovitis, ganglion cysts, tumors and other soft tissue lesions.



































































