Downloaded 622 times
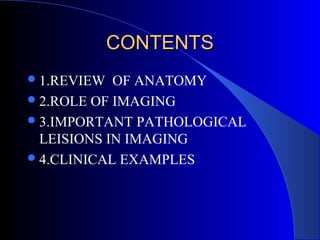
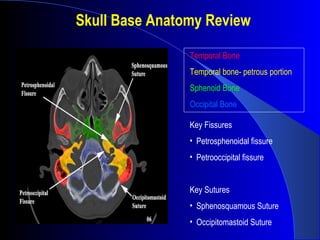
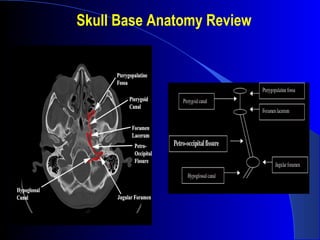
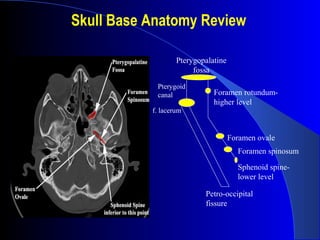


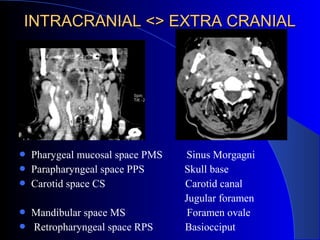
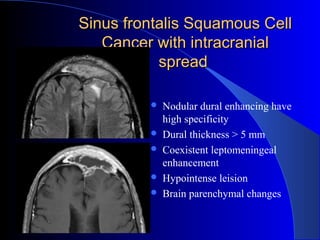
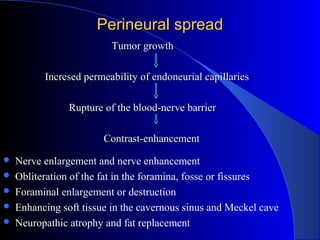
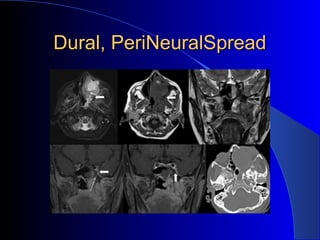
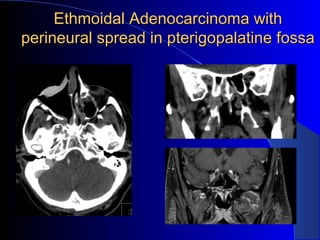
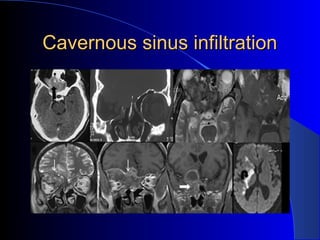
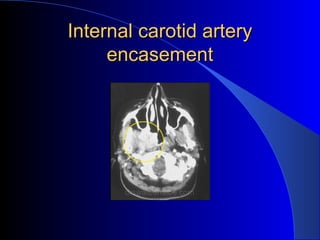


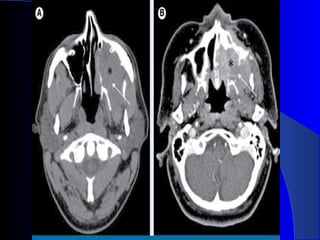

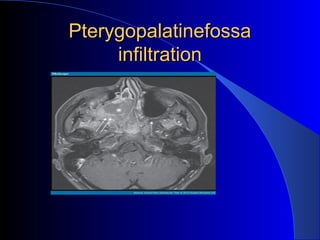
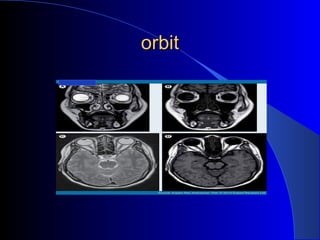
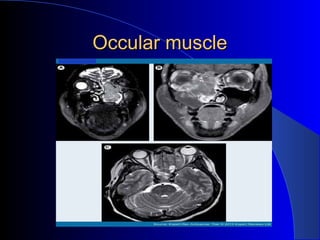
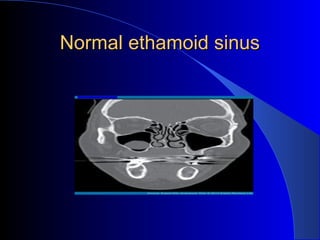
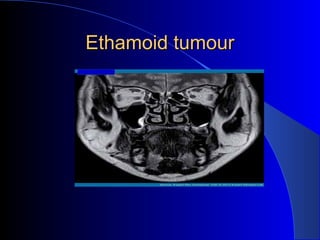
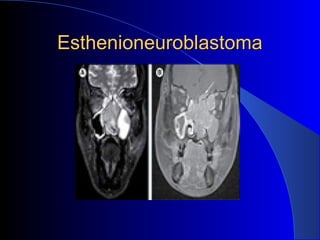
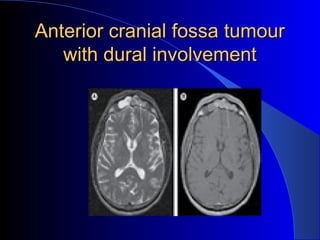
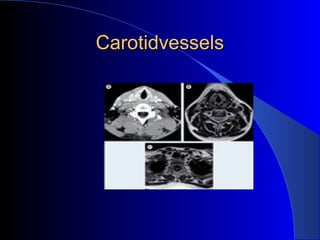
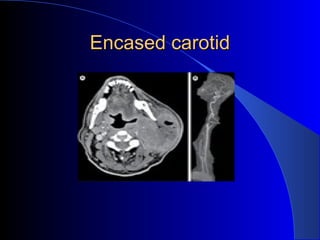
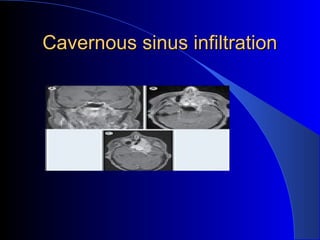

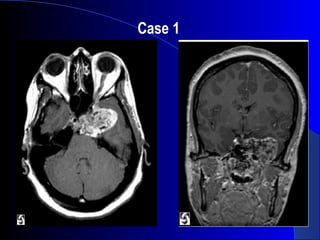
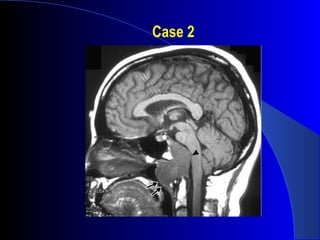
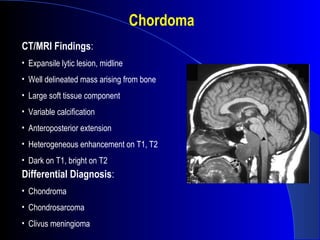
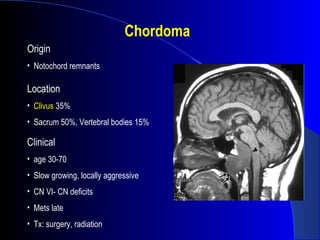
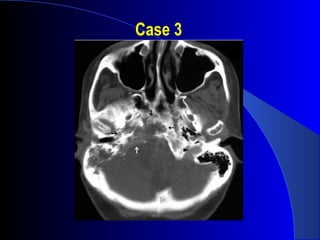
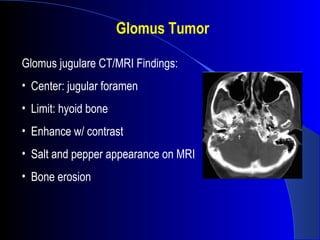
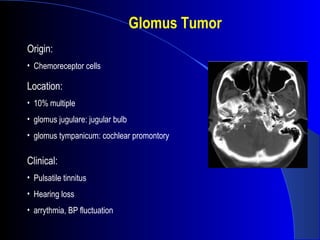


The document discusses imaging of the skull base. It begins with a review of skull base anatomy including key bones, fissures, sutures, and openings. It then covers the role of various imaging modalities like CT, MRI, and PET in diagnosing skull base lesions, determining resectability, treatment planning, and follow-up. Examples of imaging findings for conditions like sinonasal malignancy, perineural spread, and cavernous sinus infiltration are provided. Criteria for non-resectability are outlined. Common skull base pathologies are listed along with examples of three clinical cases.




















































































