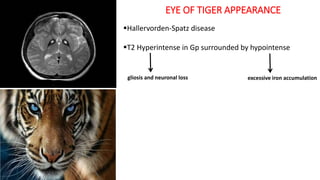
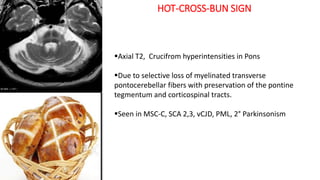
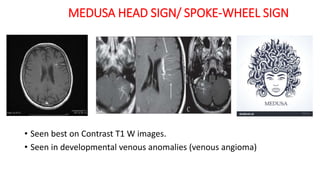
This document provides an overview of various neuroimaging signs and findings. It describes signs seen on MRI that are characteristic of different neurological conditions. Some examples included are the "eye of tiger appearance" seen in Hallervorden-Spatz disease, the "hot-cross-bun sign" seen in various spinocerebellar ataxias, and the "putaminal slit sign" seen in multiple system atrophy. It also provides images and descriptions of signs seen in conditions like multiple sclerosis, Parkinson's disease, Wilson's disease, tuberculomas, and more. The document serves as a reference for neuroradiologists and neurologists to identify various pathologies based on their imaging appearance.

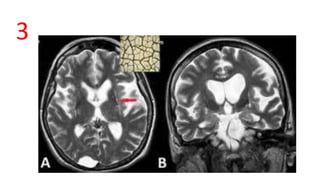

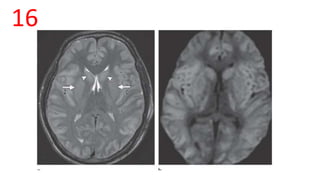
![lentiform fork sign
• A bright hyperintense rim delineates the lateral
(external capsule, long arrow) and medial boundaries
(external medullary lamina [short arrow] and internal
medullary laminae [thin arrow]) of both putamina. The
globus pallidus is divided into 2 parts by the internal
medullary laminae, which can be seen in pathologic
conditions on MR images.
• Focal restricted diffusion seen
• Seen in – metabolic acidosis – AKI, metformin,
methanol, HHS](https://image.slidesharecdn.com/imaging-spotters-190120115223/85/Imaging-neurology-spotters-29-320.jpg)





























































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)



























