Downloaded 977 times







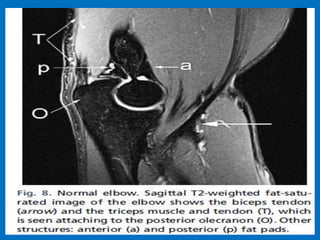








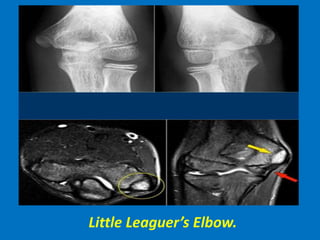

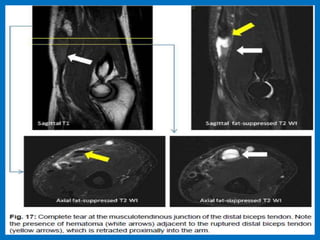
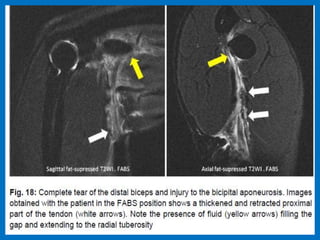






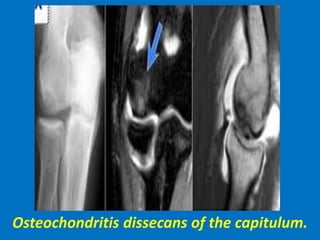

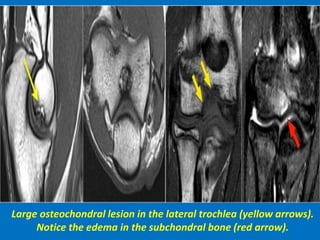
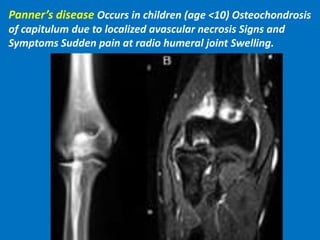

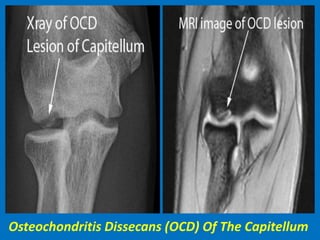







This document provides an overview of MRI techniques for imaging the elbow joint and describes various normal and pathological findings. Key points include: 1. MRI is useful for evaluating bone marrow edema, ligament and tendon injuries, cartilage defects, bursitis, and nerve entrapment around the elbow joint. 2. Common elbow injuries discussed include ulnar collateral ligament tears, lateral epicondylitis, osteochondritis dissecans, and triceps tendon avulsions. 3. Elbow arthropathies such as rheumatoid arthritis, osteoarthritis, and loose bodies can also be identified on MRI.























































































