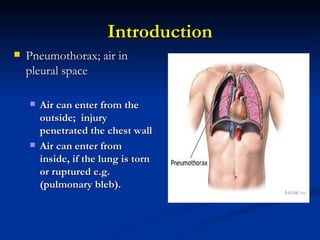
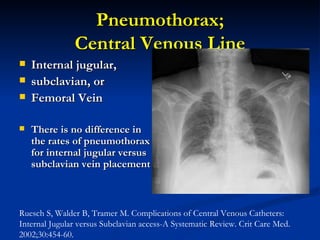
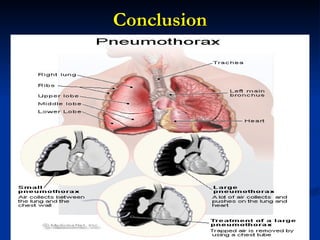
Pneumothorax is common in the ICU and can be difficult to diagnose. It has many potential causes including mechanical ventilation, procedures like central line placement, and underlying lung disease. Symptoms include chest pain and shortness of breath. Portable chest x-rays may miss pneumothorax so ultrasound is useful for diagnosis. Treatment involves chest tube placement and monitoring for complications like tension pneumothorax. Outcomes depend on severity of pneumothorax and underlying condition.






















































![Copy_of_Pneumothorax_Presentation[1] ERICA.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/copyofpneumothoraxpresentation1erica-250518100107-d43e242a-thumbnail.jpg?width=640&height=640&fit=bounds)