SURVEY OF TURKISHPRACTICE
EVALUATING THE MANAGEMENT OF
POSTDURAL PUNCTURE HEADACHE
IN THE OBSTETRIC POPULATION
Berrin Günaydın, MD, PhD
Department of Anesthesiology
Gazi University Faculty of Medicine
ANKARA-TURKEY
Background
• Surveys andmeta-analysis concerning
the management of PDPH in the
obstetric population have been published
– Choi et al. Examining the evidence in anaesthesia literature: a
survey and evaluation of obstetrical Postdural puncture
headache reports. Can. J. Anesth., 49, 49–56, 2002.
– Baraz and Collis. The management of accidental dural
puncture during labour epidural analgesia: a survey of UK
practice. Anaesthesia, 60, 673-679, 2005.
5.
Aim
• Primarily todetermine the current practice in the
management of PDPH in a small sample
reflecting roughly the commonly preferred
approaches
• Secondly to provide awareness of the
responders with this particular entity
6.
Methods
• Questionnaire including24 questions similar to
Baraz and Collis’s were given to the
participants
• Participants were asked to submit their
surveys either to the surveyors or send it via e-
mail to the contact person later
• Microsoft Excel® software was used for data
analysis
• Results were presented as n and/or %
Results
• 78 outof 111 surveys returned
(Response rate was 70%)
• The responders consisted of
– 21 (26.92%) residents
– 25 (32.05%) fellows
– 21 (26.92%) academic staff
– 11 (14.10%) did not identify any degree
9.
Results
• Rate ofauditing inadvertent dural puncture
during labour or cesarean was 35%
• Having written guidelines for the
management of accidental dural puncture
– Yes: 10%
– N: 64%
– Under the process of writing: 4%
– No reply: 22%
50% stated that it
was necessary at
the end of the survey
10.
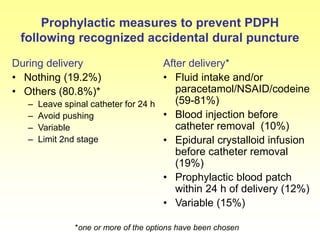
Prophylactic measures toprevent PDPH
following recognized accidental dural puncture
During delivery
• Nothing (19.2%)
• Others (80.8%)*
– Leave spinal catheter for 24 h
– Avoid pushing
– Variable
– Limit 2nd stage
After delivery*
• Fluid intake and/or
paracetamol/NSAID/codeine
(59-81%)
• Blood injection before
catheter removal (10%)
• Epidural crystalloid infusion
before catheter removal
(19%)
• Prophylactic blood patch
within 24 h of delivery (12%)
• Variable (15%)
*one or more of the options have been chosen
11.
Results - Duringdelivery
• When accidental dural puncture during
epidural insertion was recognized
– epidural catheter was left in situ to use as a
spinal catheter (36%)
Kuczkowski K.M., Decreasing the incidence of post-dural puncture headache: an update. Acta
Anaesthesiol. Scand., 49, 594, 2005.
or
– epidural catheter was re-sited at a different
level (64%)
Gunaydin and Karaca. Prevention strategy for PDPH. Acta Anaesth. Belg., 57, 163-165, 2006.
12.
Possible reasons forusing an epidural
catheter as an intrathecal catheter
No recommendation (62%)
Possible reasons according to preferance order (38%)*
Allow immediate analgesia for labour
Avoid another dural puncture
Reduce the incidence and/or severity of PDPH
Only in difficult cases (e.g. obesity & multiple attempts)
Kuczkowski K.M., Post-dural puncture headache in the obstetric patient: an old problem. New solutions.
Minerva Anestesiol., 70, 823-830, 2004.
Kuczkowski and Benumof. Decrease in the incidence of post-dural puncture headache: maintaining CSF
pressure. Acta Anaesthesiol. Scand., 47, 98-100, 2003.
*one or more of the options have been chosen
13.
Results - Afterdelivery
Non-invasive methods for PDPH treatment
• In addition to the encouragement of fluid intake
and/or paracetamol/NSAID/codeine
– Caffeine (oral/iv)
– Theophylline (oral)
– IV hydrocortisone
– IM ACTH
– SC sumatriptin
– Strong opioids
14.
Ambulation after deliveryfollowing
accidental dural puncture
• As early as possible: 7%
• Bed rest:6 h (3%),12 h (15%) or 24 h (36%)
• No idea: 49%
15.
Methods routinely usedfor PDPH treatment
• 1st option is the conservative treatment
• Blood patch was mostly preferred after failed
conservative treatment
• Blood patch as soon as PDPH diagnosed is less
preferred
• Different measures can be selected
16.
History (Gormley1960, DiGiovanni & Dunbar 1970)
Mechanism of action
Plug theory
Clot is formed by injecting 15-20 ml autologous
blood in the epidural space to provide adherence
to the dura mater and directly patches the hole
Pressure patch hypothesis
Volume of blood injected into epidural space
increases CSF pressure leading to reduction in
the traction of the pain sensitive brain structures
Epidural Blood Patch (EBP)
17.
EBP
Contraindications
Infection onthe back
Sepsis
Coagulopathy
Raised white cell
count
Prexia
Patient refusal
Timing
Beyond 24 h after
dural puncture
Recumbent
positioning
For 2 h after patching
may improve the
efficacy
18.
EBP
Complication rateis rare
~35% backache
Success rate is ~94% (70-98%)
90% initial relief
61-75% persistent relief
Repeat EBP has a similar success rate
Reverse complications of dural puncture
19.
Treatment
It isrecommended not to delay EBP more than 24 h
after the diagnosis of severe PDPH
20.
EBP
• Mostly performedin the recovery room
• Sometimes in the labour ward
• Rarely in the patient’s room
• Generally performed with the help of a
resident or a staff member
• Rarely performed by one person
Gunaydin et al. Acta Anaesthesiol Belg 2008
21.
EBP
• Intravenous accessbefore EBP (69%)
• ECG (58%)
• Blood pressure (65%) and
• Pulse oxymeter (63%) were performed by the
majority of the responders
Gunaydin et al. Acta Anaesthesiol Belg 2008
22.
Advices at dischargeafter a
successfull EBP
• Discharge
– After EBP 1 (4%), 2 (15%) or 3-6 hours (44%)
• Follow-up
– Before full mobilization 2 (47%) or 4 hours (23%)
of bed rest
– Increase fluid intake
– Keep intervention side clean
– Contact whenever headache reoccurs and report
fever, weakness or numbness
Gunaydin et al. Acta Anaesthesiol Belg 2008
23.
After an unsuccessfullEBP
• Rate of never considering another EBP (36%)
• Rate of repeating EBP (37%)
• No recommendation (27%)
• If two EBPs were unsuccessfull, further
investigations were considered (63%)
Gunaydin et al. Acta Anaesthesiol Belg 2008
24.
Conclusion
• According tothe present survey, re-siting
epidural catheter at a different intervertebral
space or using epidural catheter as an
intrathecal catheter was preferred for the
prevention of PDPH in case of recognized
accidental dural puncture
• Non-invasive methods consisting of
encouragement of fluid intake and drugs were
routinely used for the treatment of PDPH
25.
Conclusion
• Although theseresults showed the current
practice of this small sample, in order to
follow the change in these strategies and
to catch almost a standard approach for
the prevention and management of PDPH,
further surveys including most of the
centers are required.