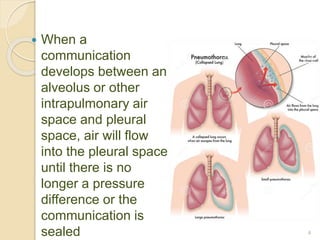
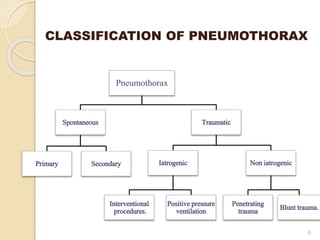
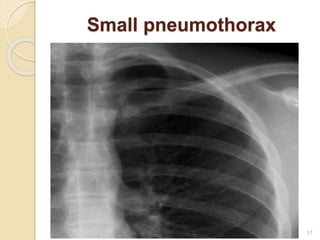
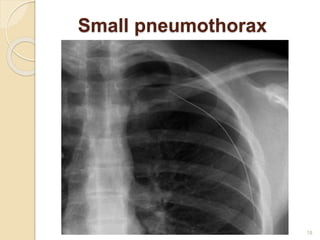
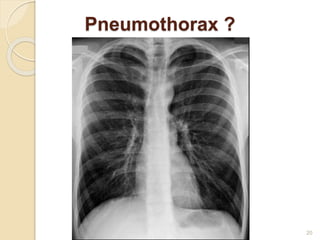
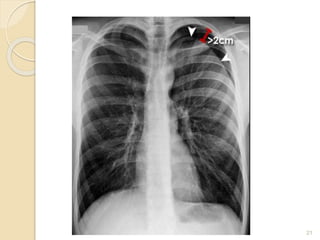
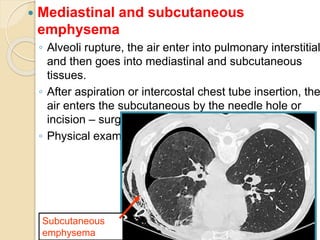
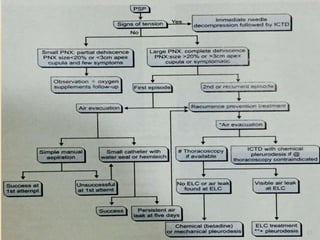
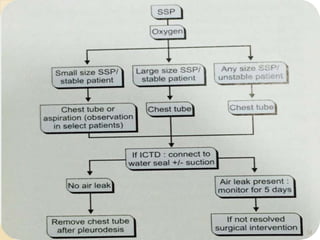
Pneumothorax is the presence of air or gas in the pleural space between the lung and chest wall. It occurs when there is a communication between an alveolus or air space and the pleural space, allowing air to enter the pleural space. Pneumothoraces are classified as spontaneous (primary or secondary), traumatic, or iatrogenic. Treatment depends on the type and severity but may include observation, oxygen therapy, needle aspiration, chest tube drainage, chemical pleurodesis, or surgery. Complications can include infection, bleeding, or mediastinal and subcutaneous emphysema.