Downloaded 471 times







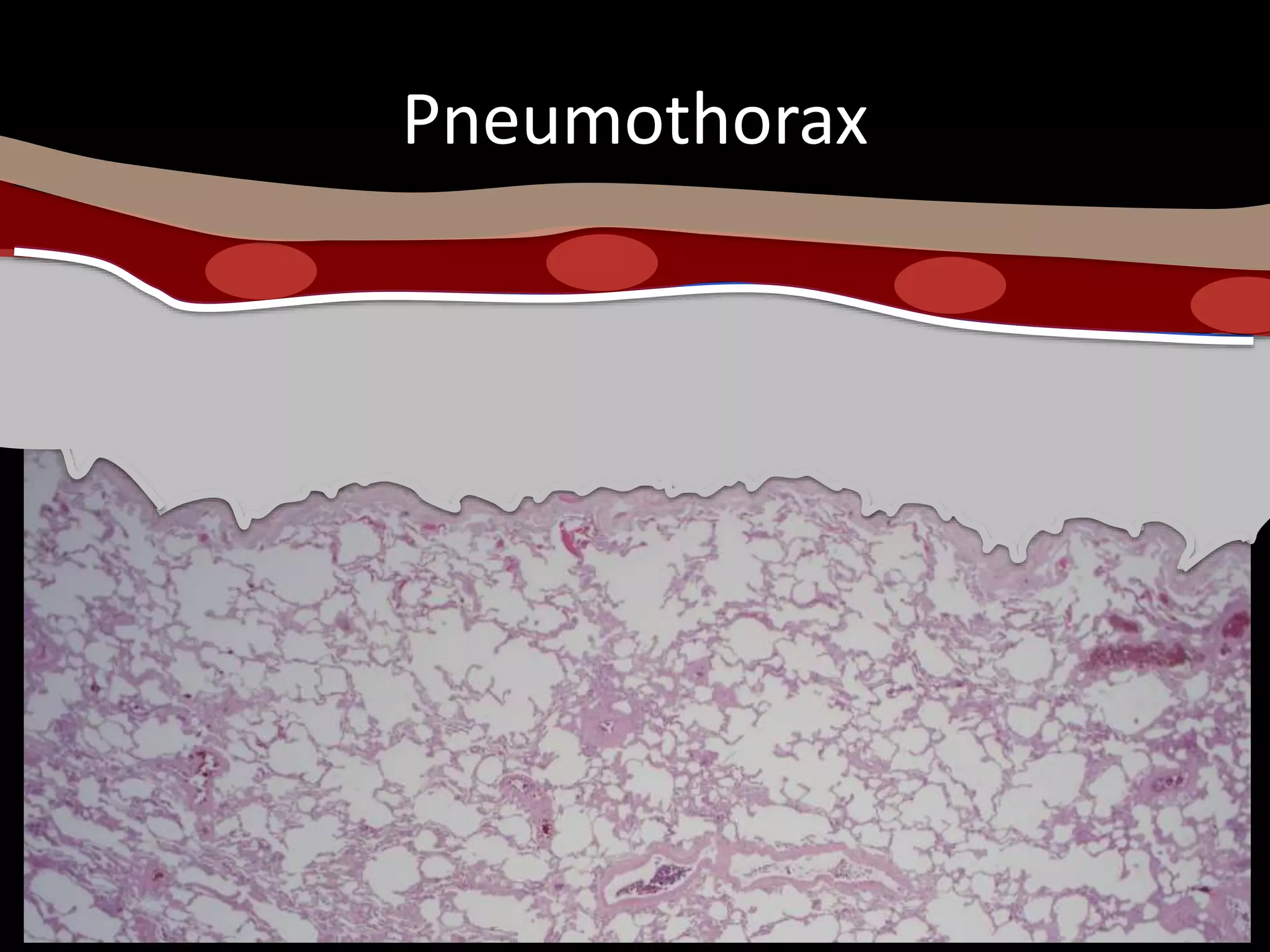
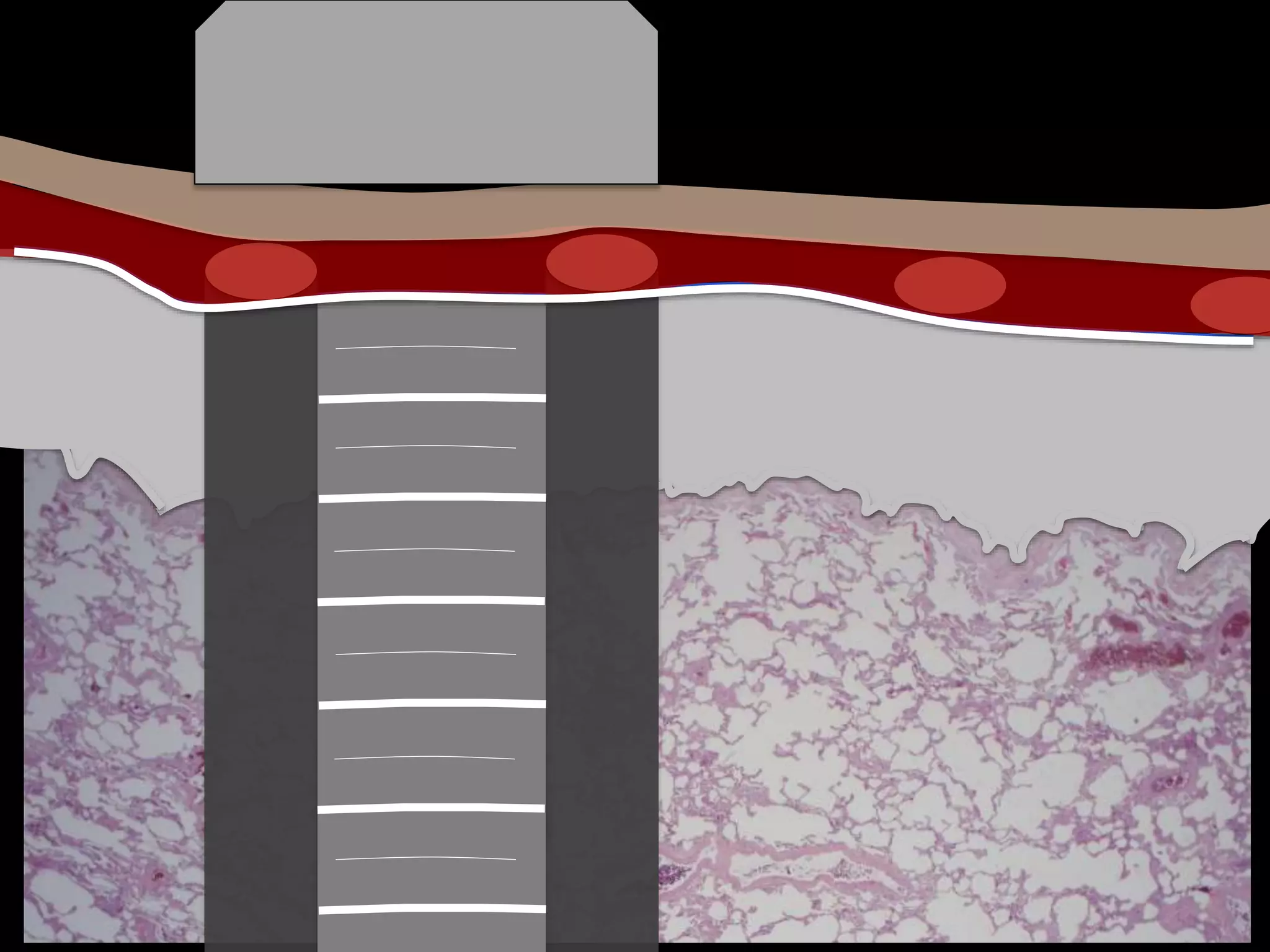

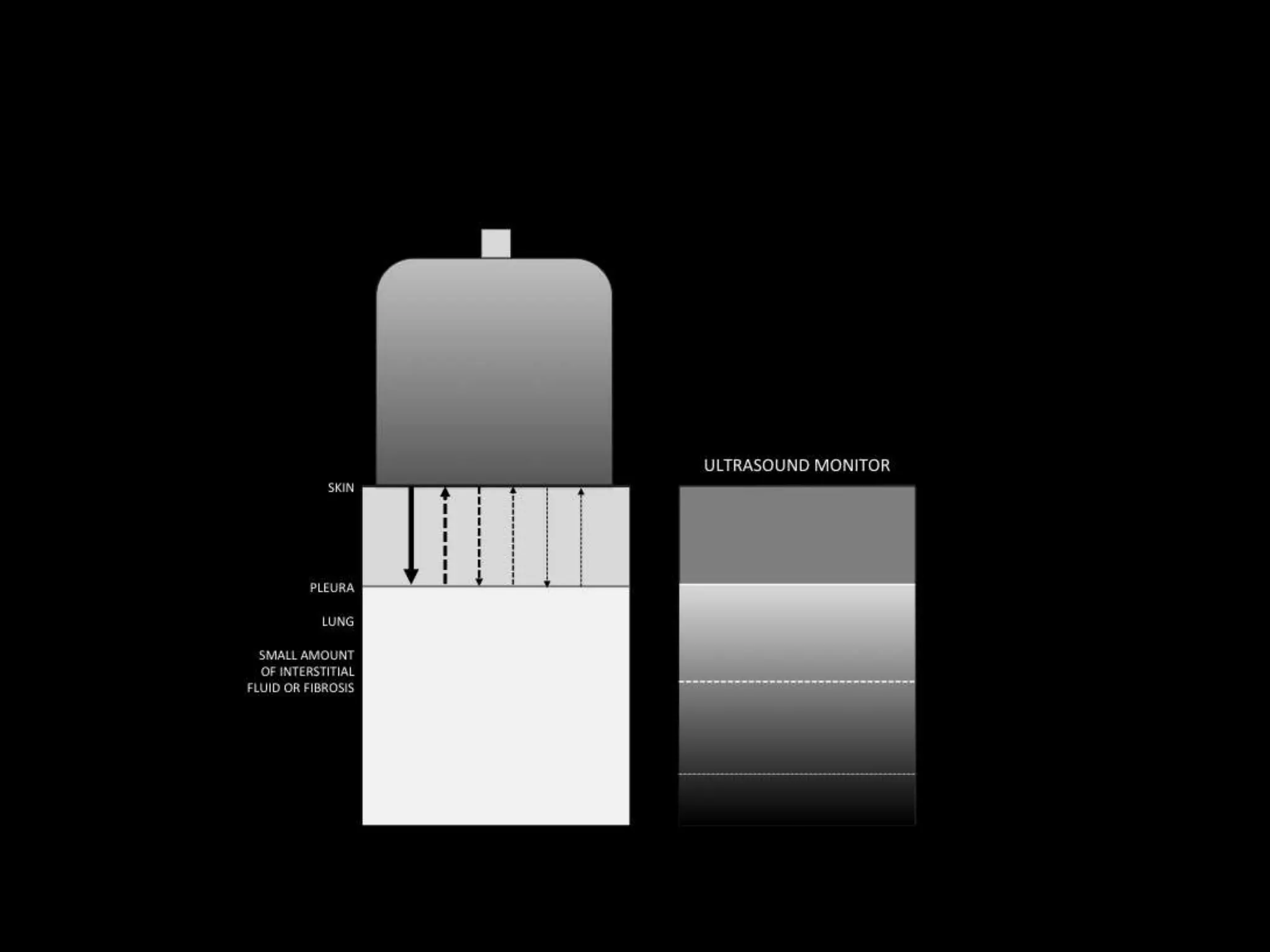






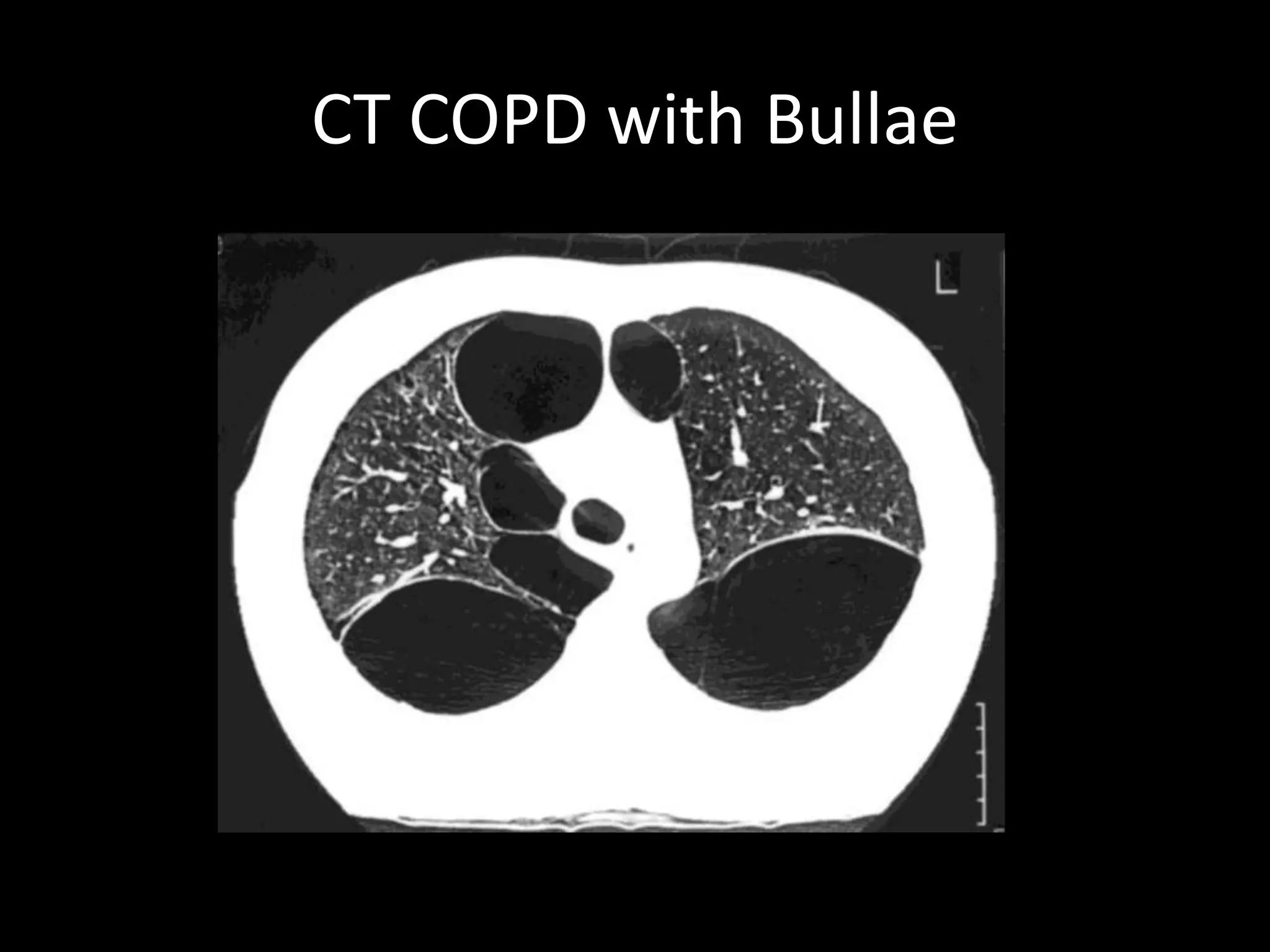
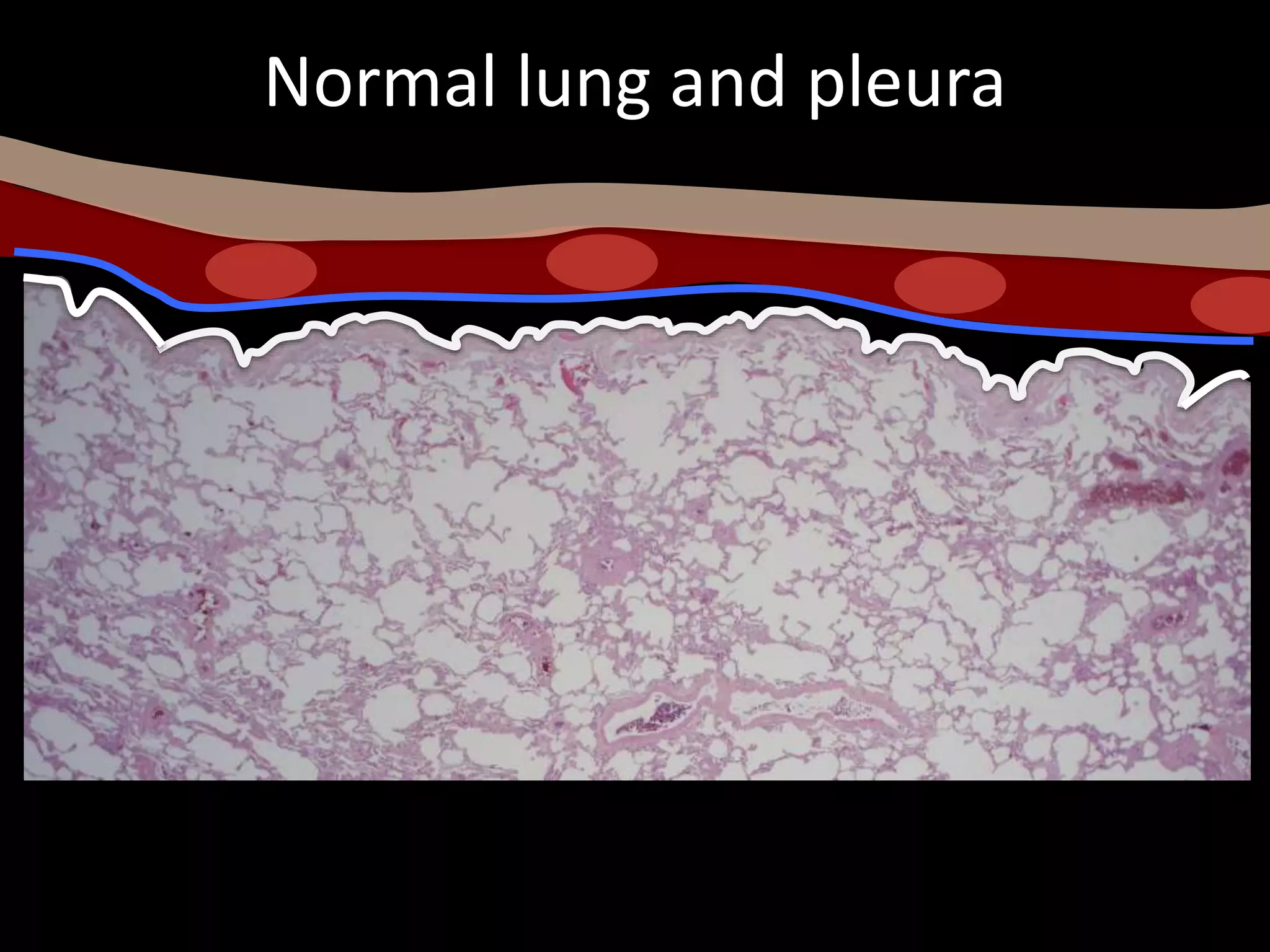
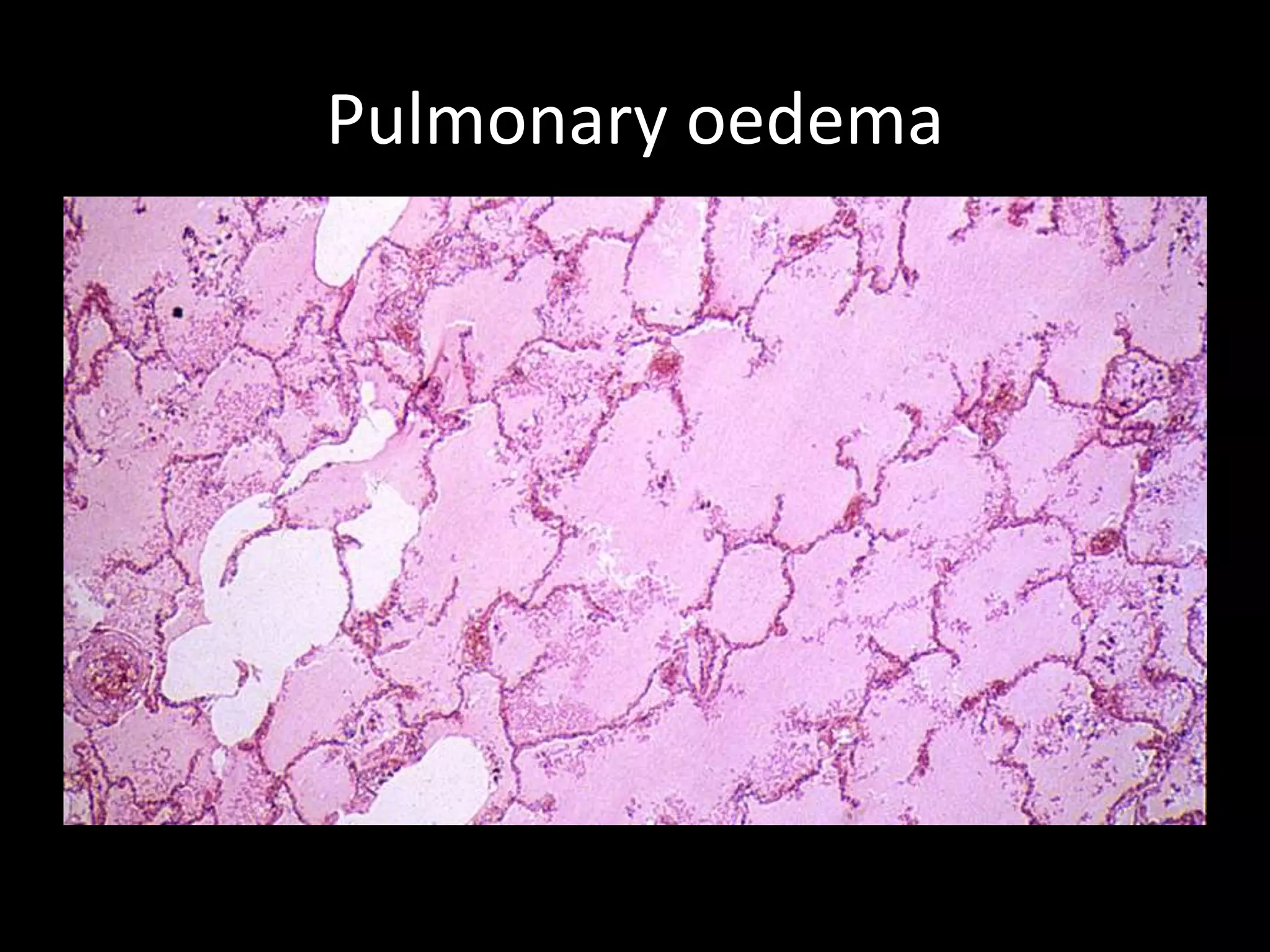

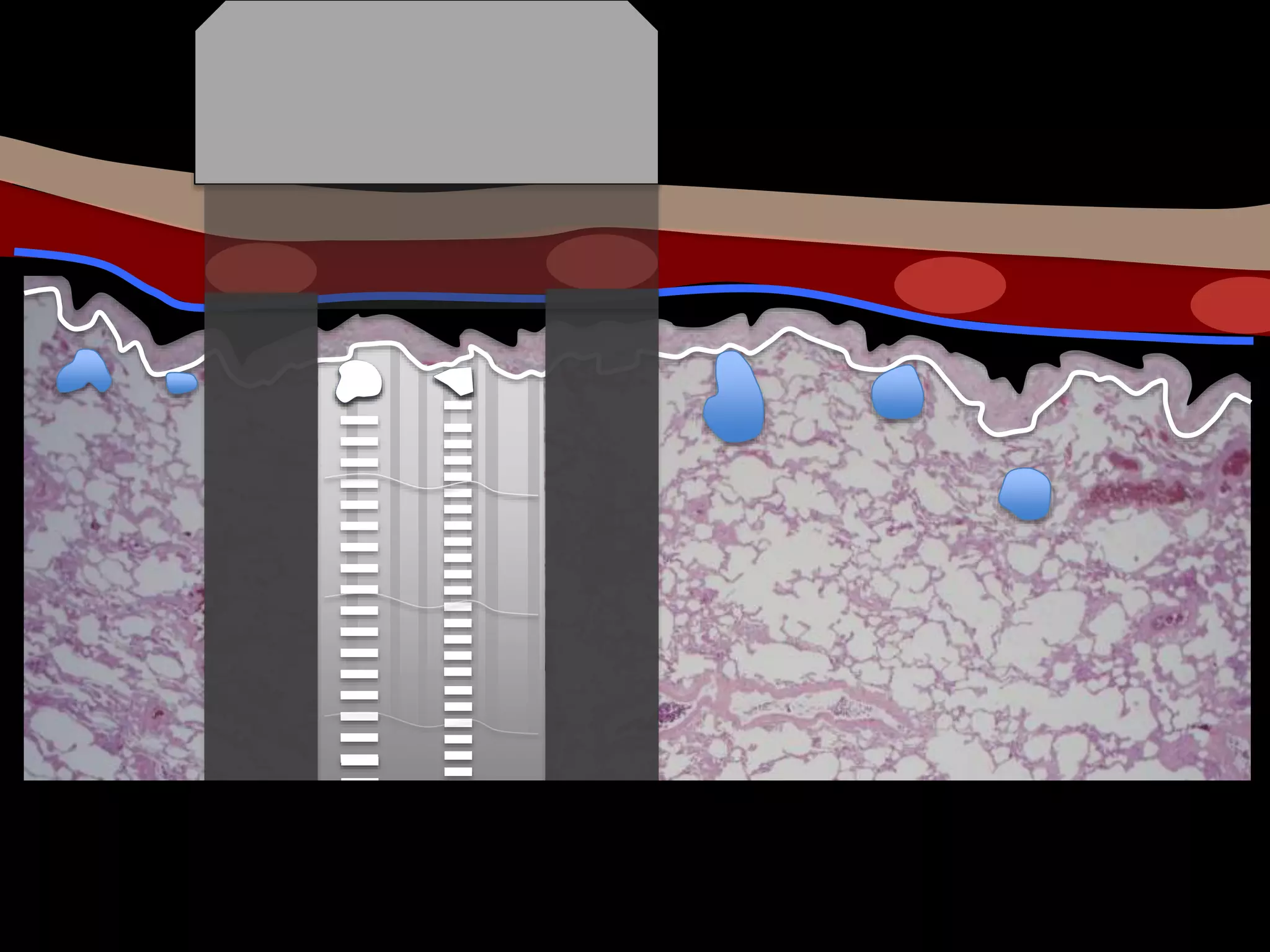

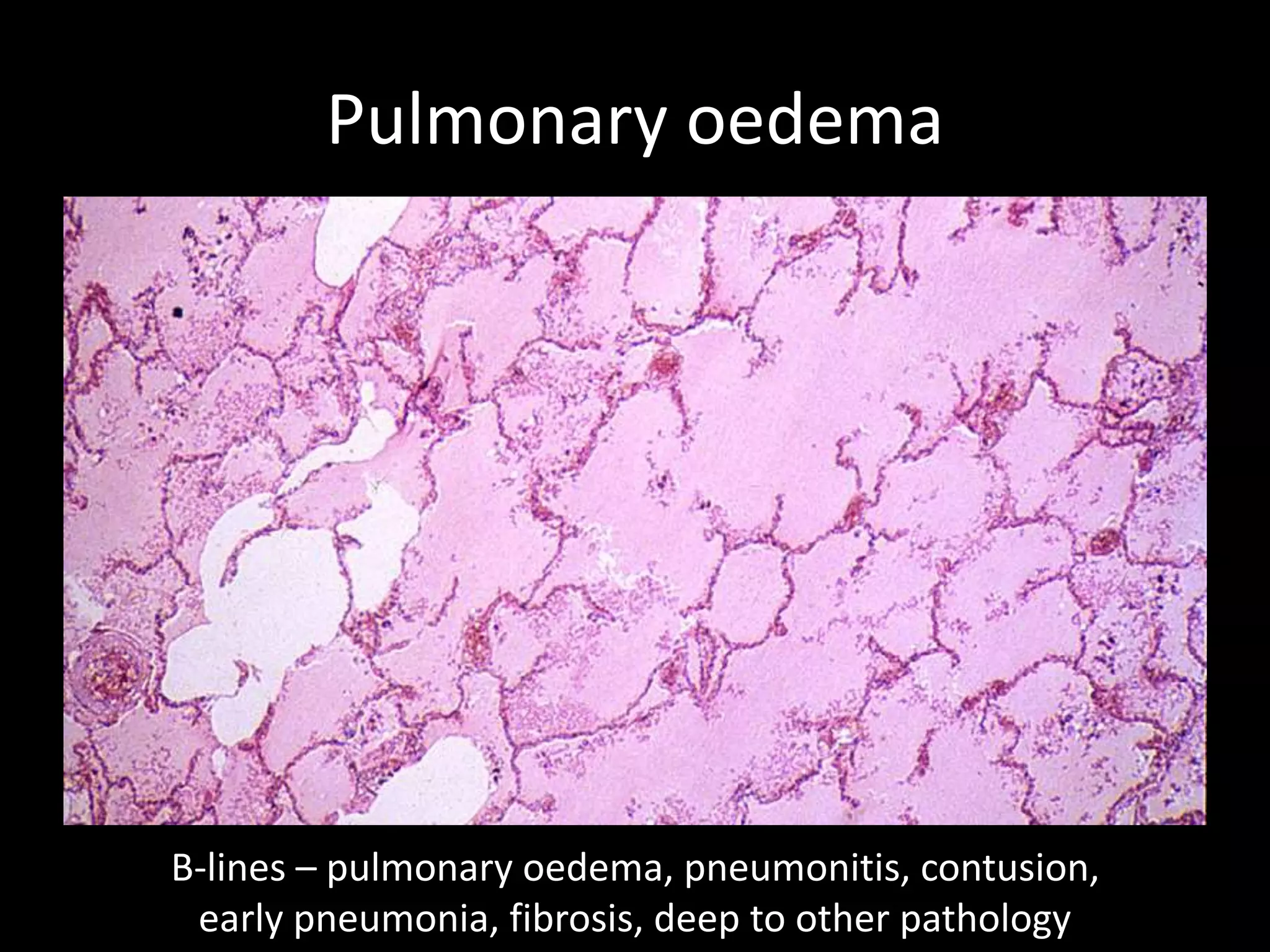


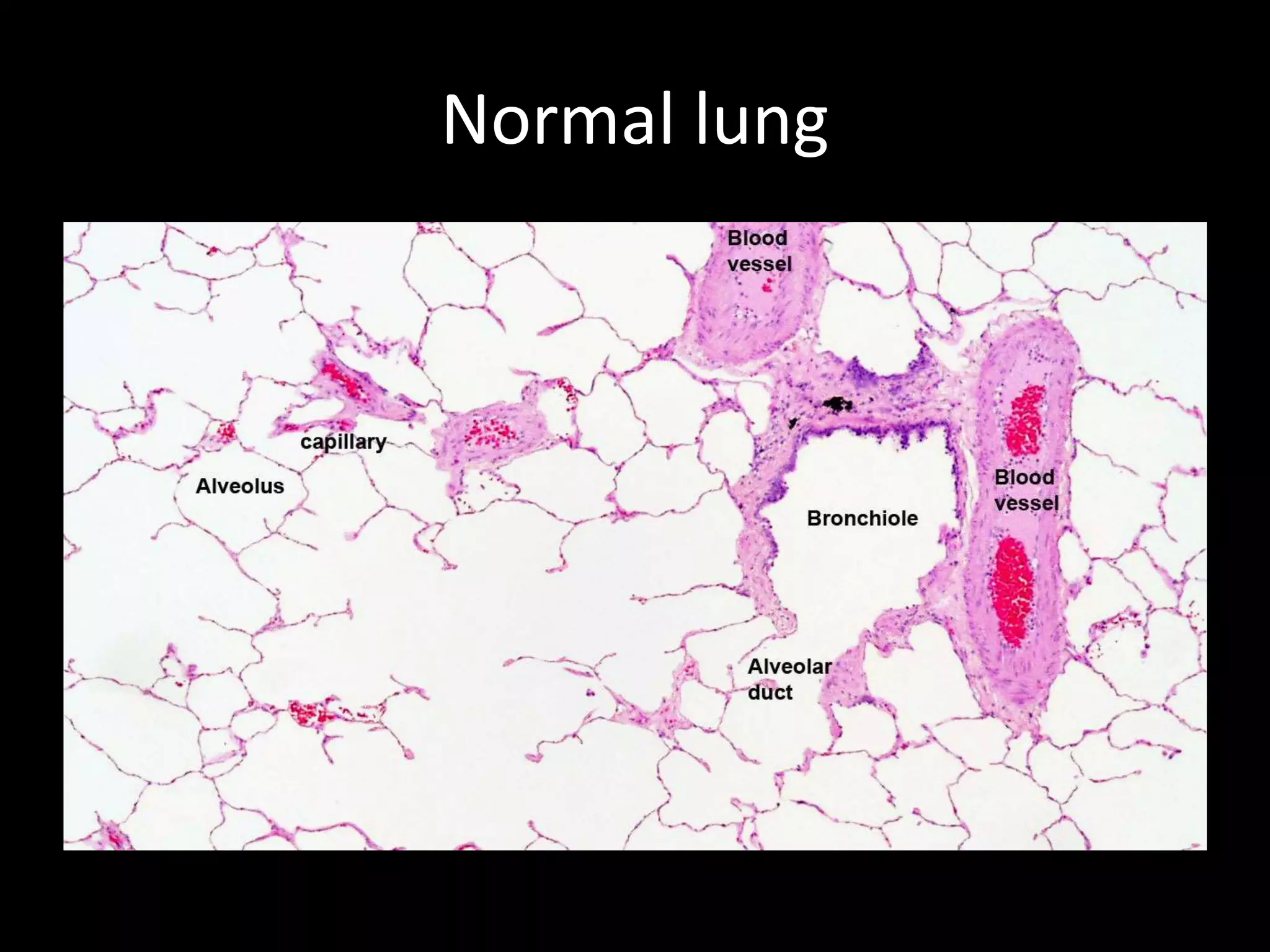

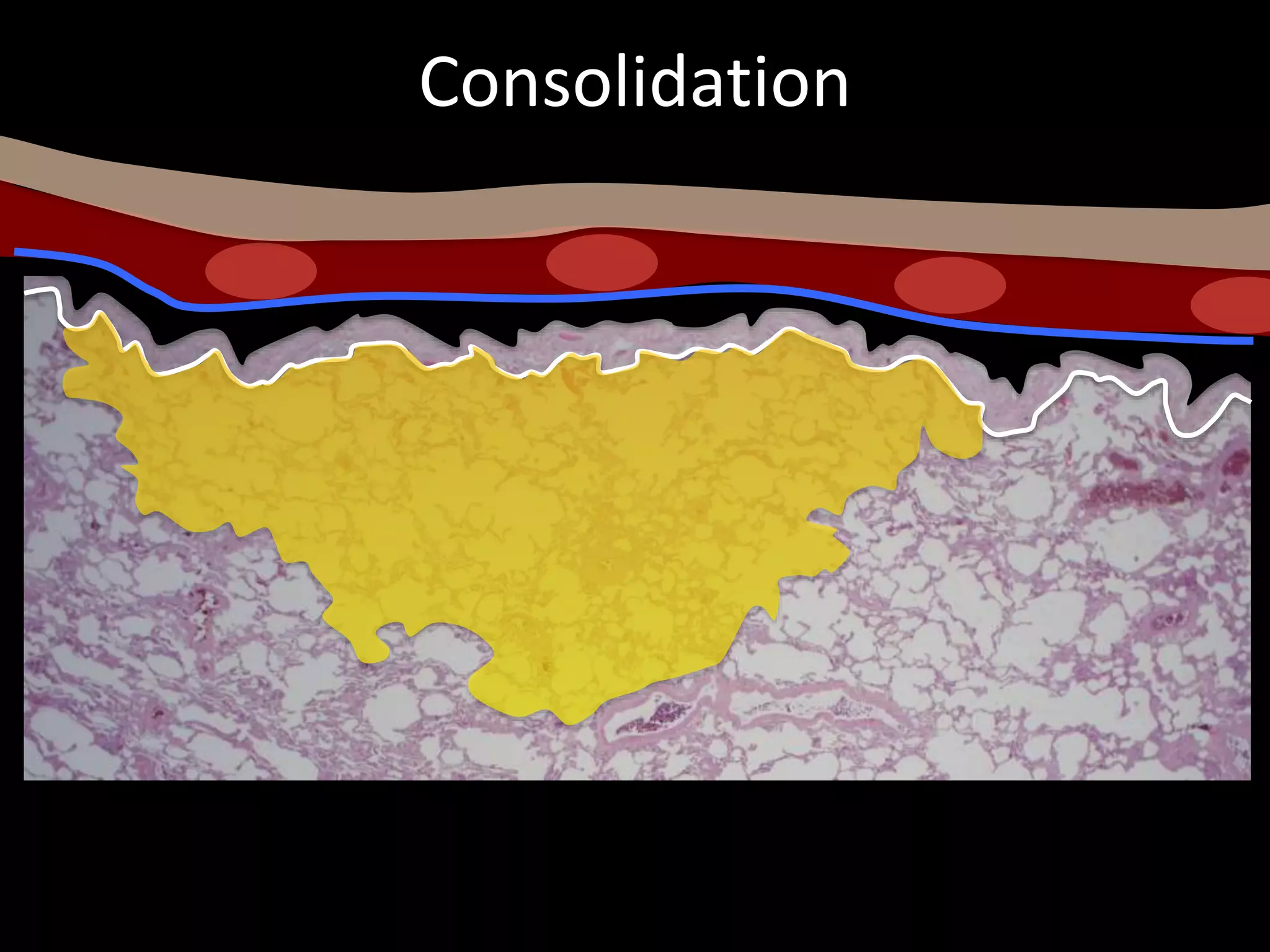
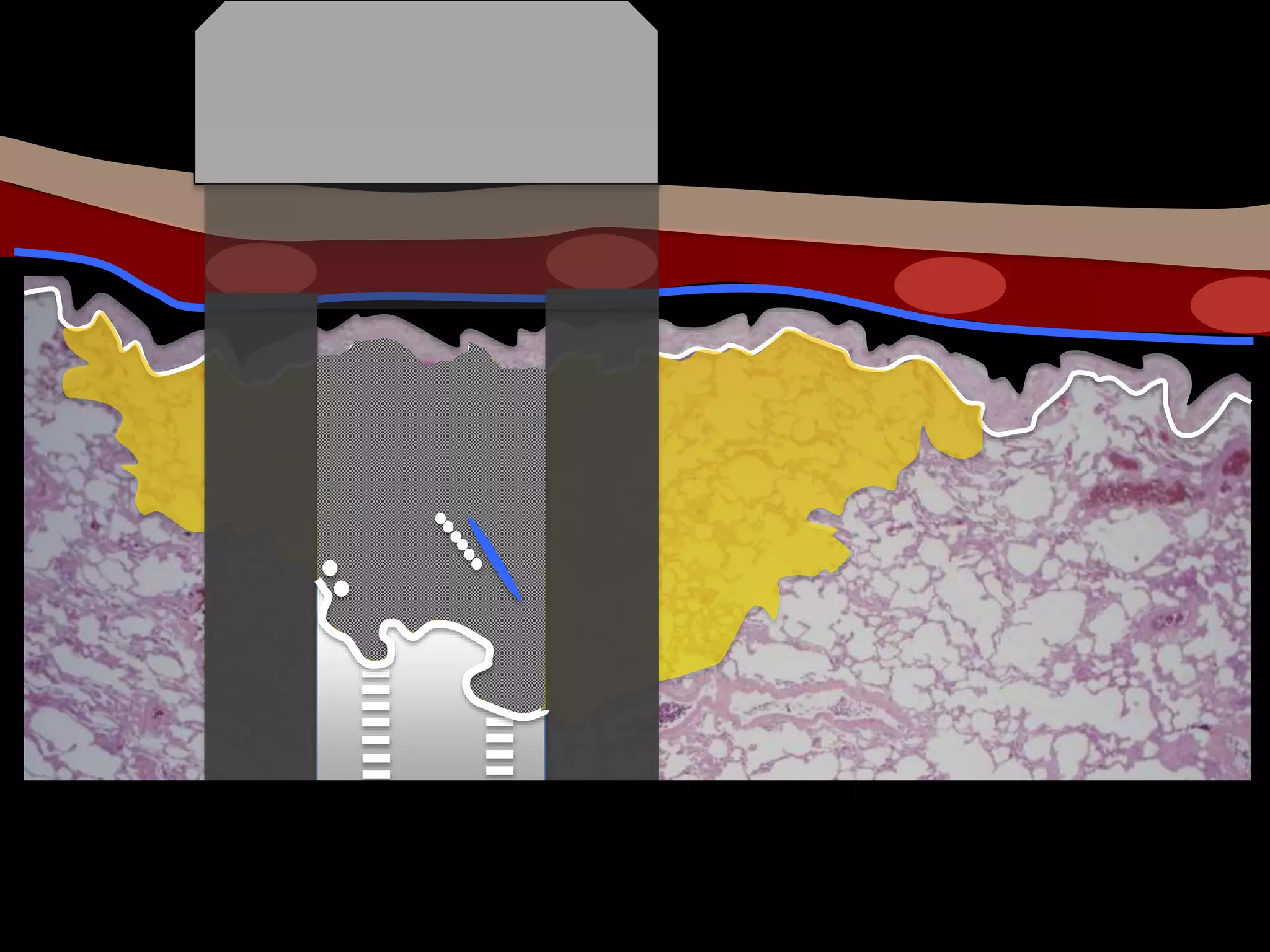






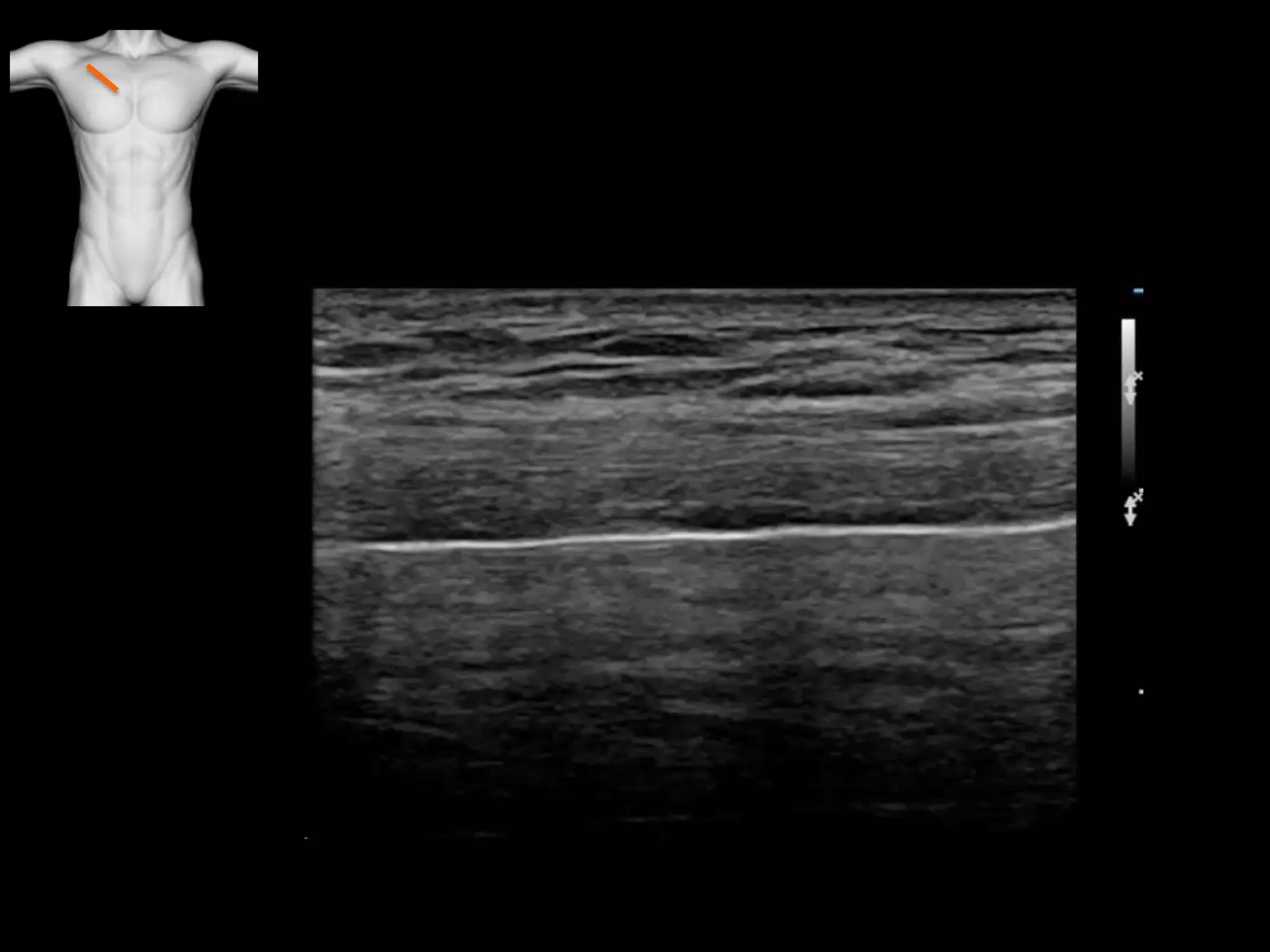










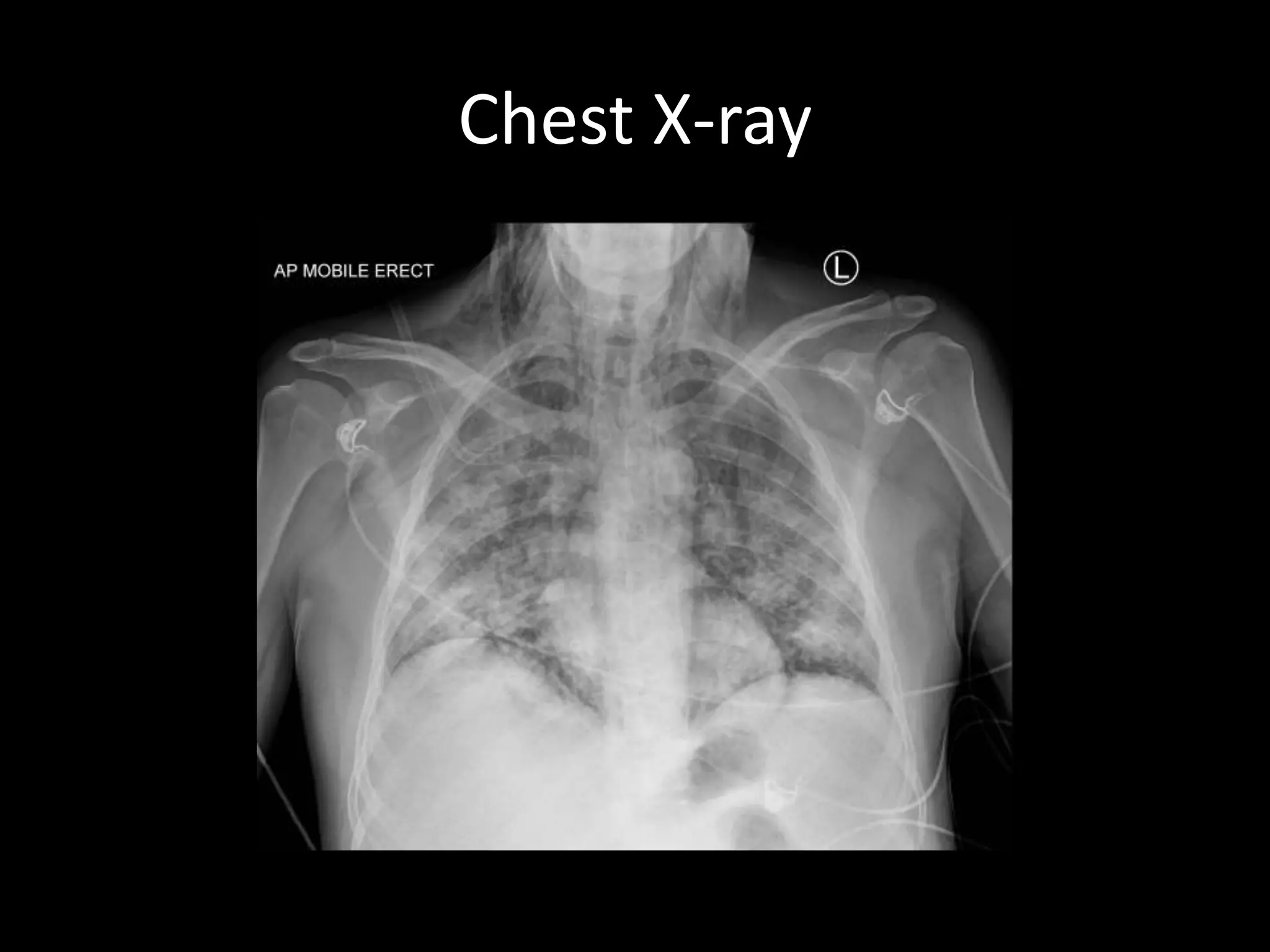


















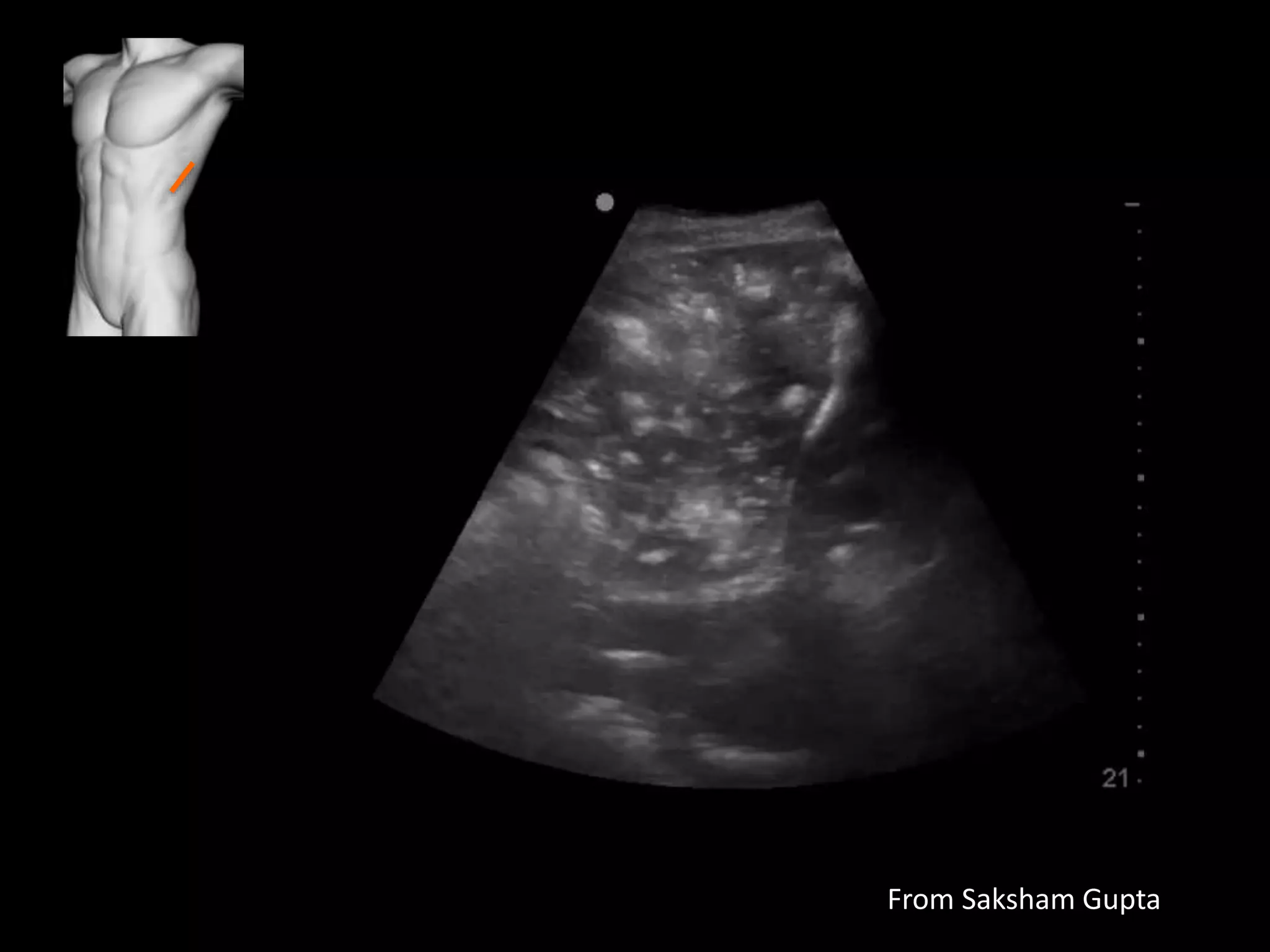



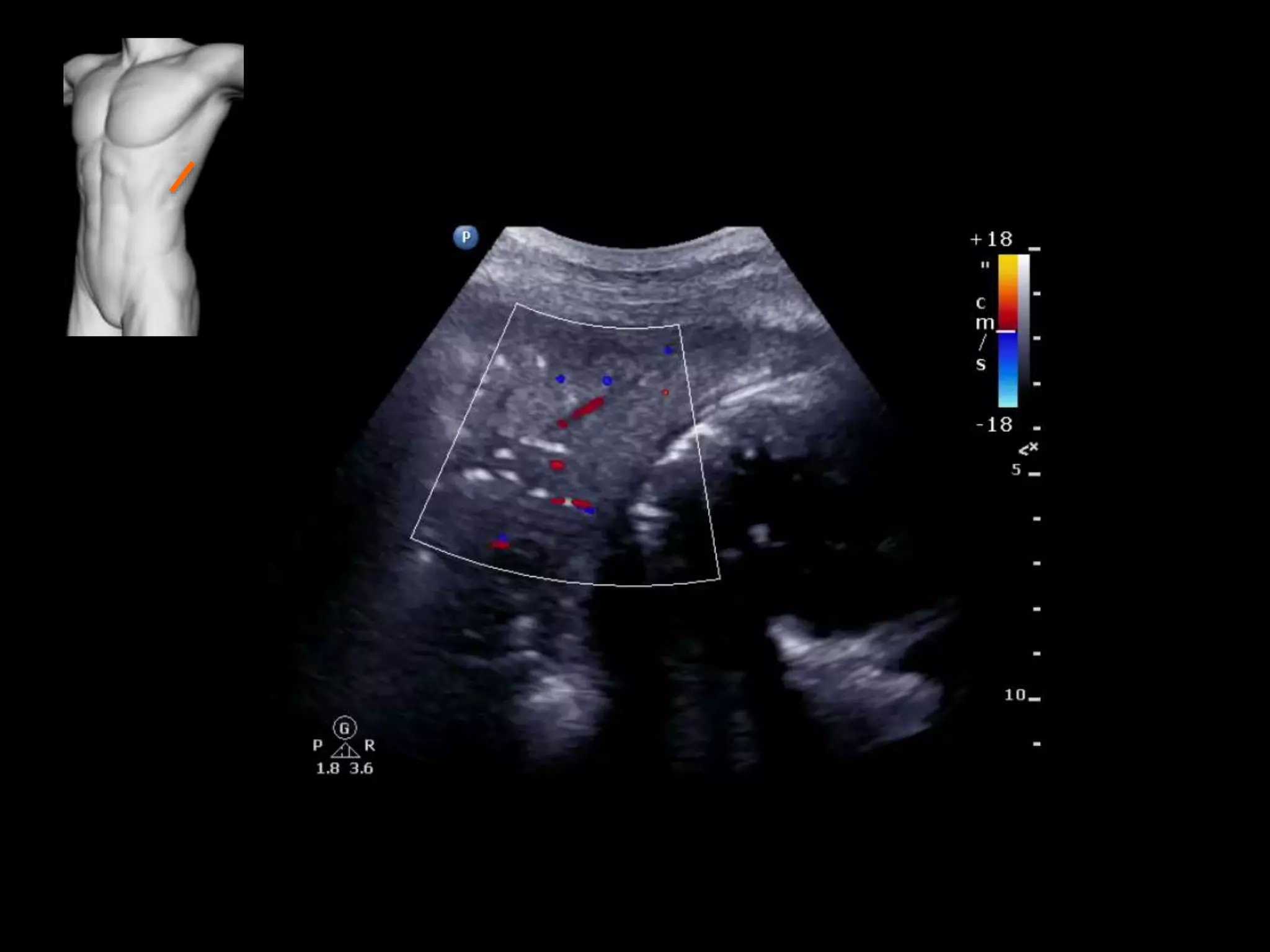


















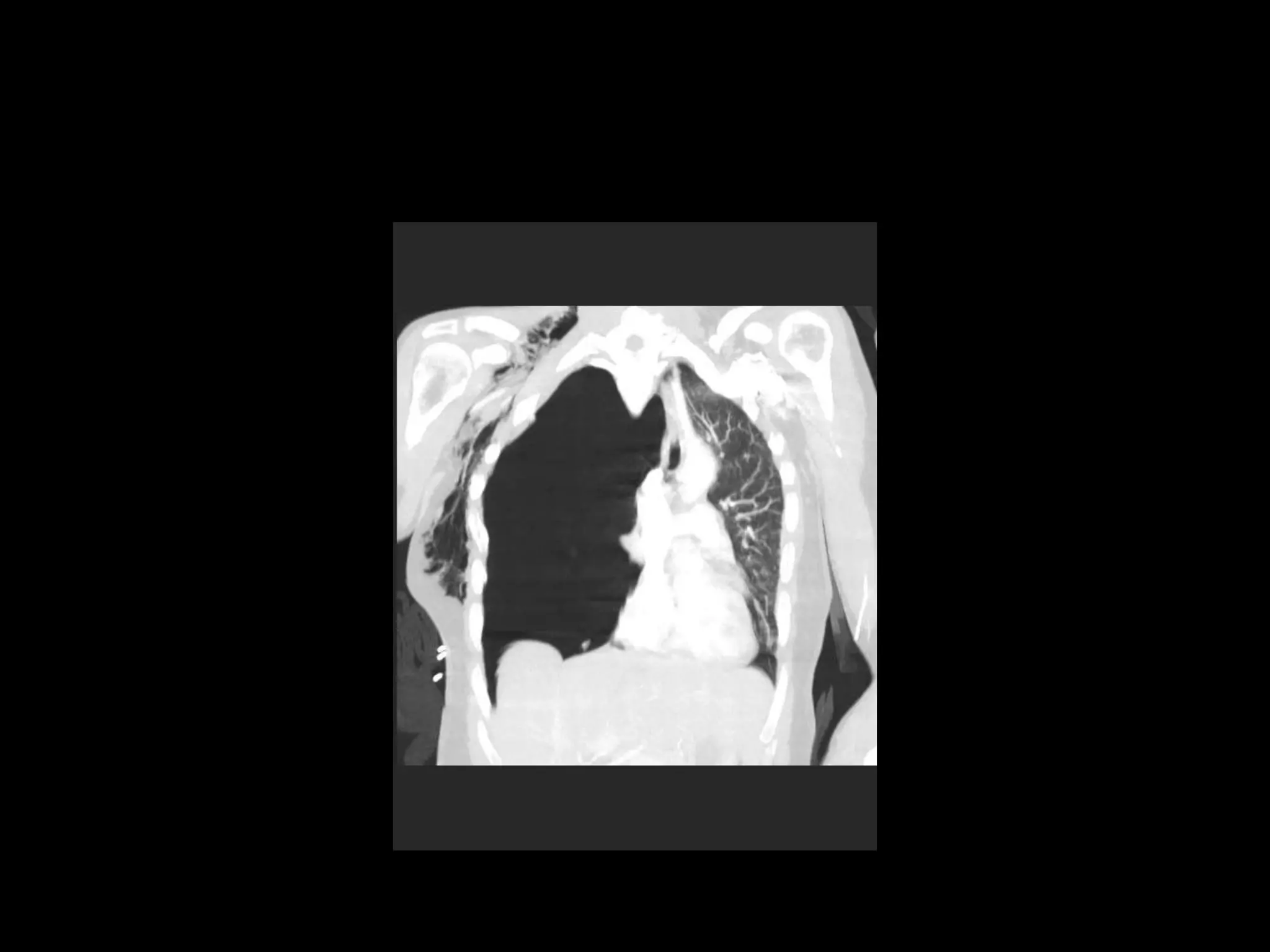















This document provides an overview of lung ultrasound and discusses various lung pathologies that can be identified using ultrasound. It begins with background on lung anatomy and ultrasound principles. Various normal and abnormal findings are then described, including pneumothorax, pulmonary edema, consolidation, pleural effusions, and lung tumors. Case studies are presented to demonstrate ultrasound identification of conditions like emphysema, pneumonia, pulmonary edema, pneumothorax, and lung cancer. The document emphasizes that lung ultrasound allows accurate diagnosis of many lung conditions at the point of care based on visualization of artifacts, B-lines, lung sliding, and consolidations.























































































