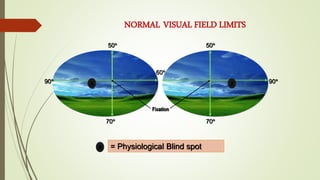
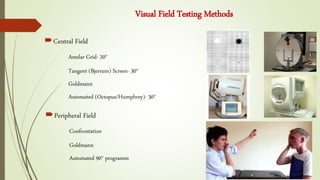
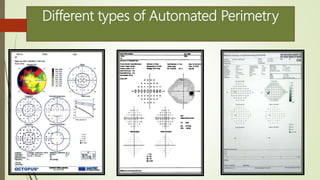
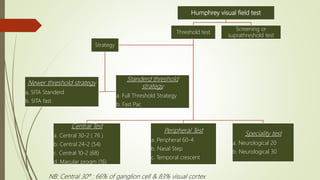
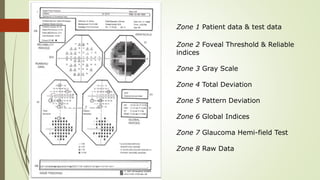
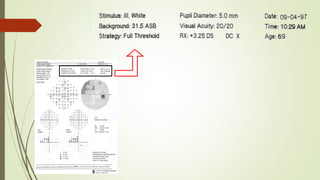
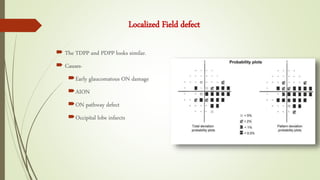
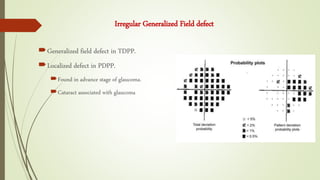
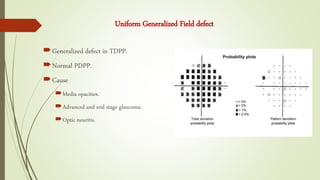
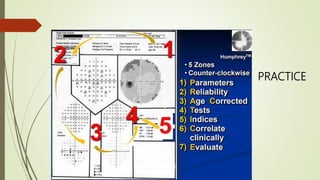
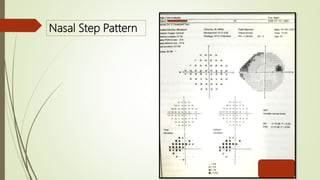
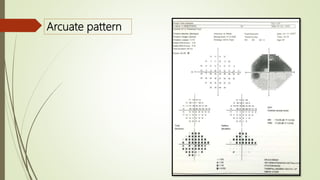
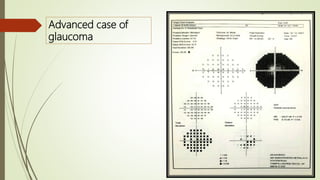
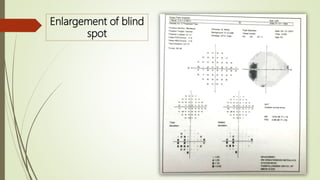
Perimetry is a test that measures the visual field and is important for diagnosing and managing glaucoma. There are two main types of perimetry - kinetic and static. The Humphrey visual field test is a type of static, automated perimetry that uses thresholds to test the central and peripheral visual field. It provides reliable indices and plots like total deviation and pattern deviation to analyze visual field defects and monitor for progression of glaucoma. Common visual field defects seen in glaucoma include localized defects, arcuate scotomas, nasal steps, and advanced defects like tunnel vision.