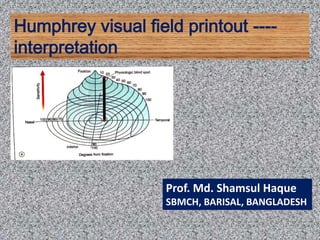
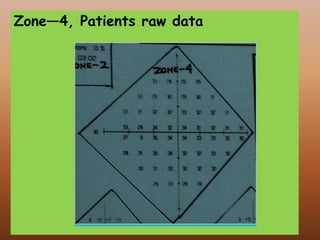
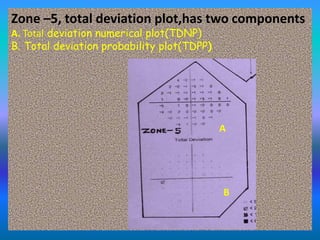
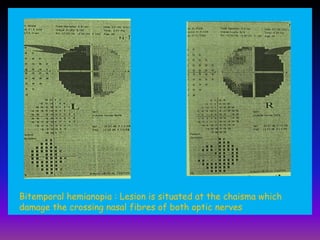
The document provides a comprehensive interpretation of the Humphrey visual field test, detailing its methodology, types of perimetry, testing strategies, and classification of visual field defects. It explains two main types of threshold tests and the eight zones of the test printout, including various parameters for assessing glaucoma and neurological lesions. Additionally, the document covers specific visual field defects, diagnosis techniques, and case studies illustrating various conditions affecting visual perception.