Downloaded 378 times
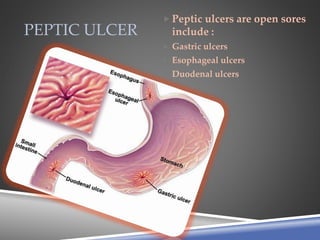
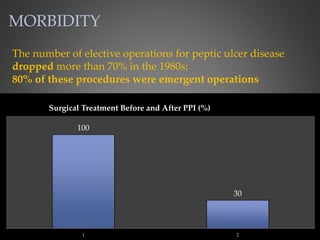

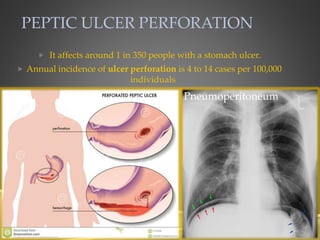
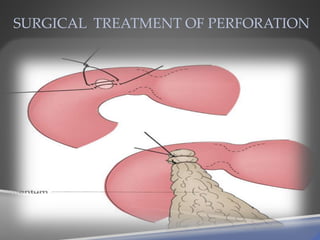
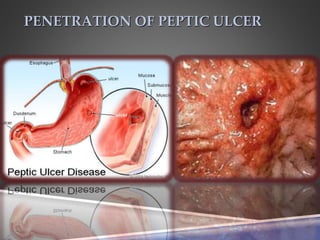
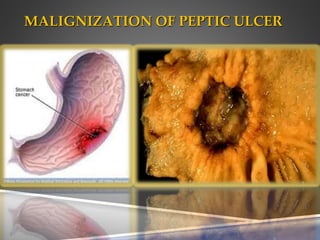
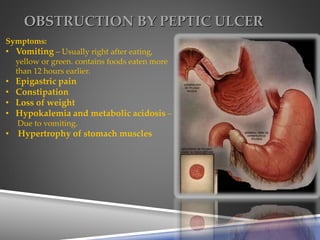
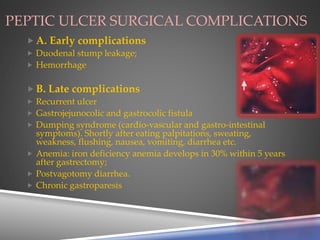



Peptic ulcer disease includes gastric, esophageal, and duodenal ulcers, with complications such as perforation, bleeding, and obstruction. The incidence of elective surgeries for peptic ulcers has decreased significantly, with internal bleeding being a common complication. Risk factors include NSAID use, age, and genetic predisposition, and symptoms of complications can include sharp pain, black stools, and vomiting.
































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


