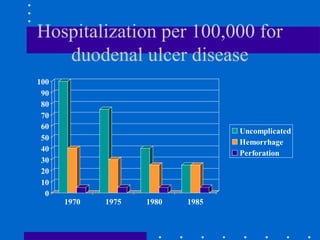
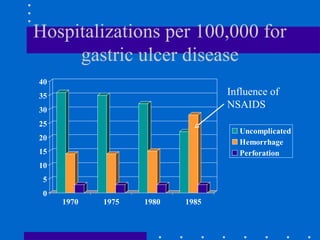
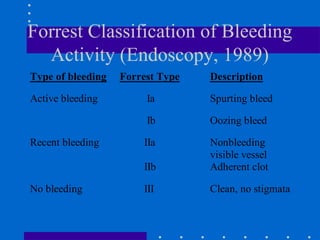
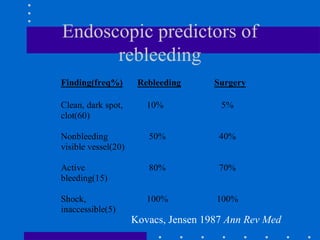
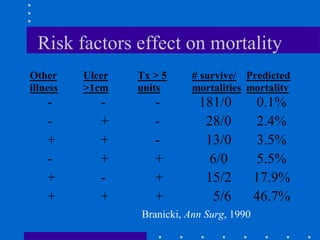
This document summarizes the surgical management of complications from peptic ulcer disease. It discusses the trends in hospitalizations for ulcer disease over time, predictors of rebleeding, and the value of endoscopic treatments. For bleeding ulcers, the choice of operation depends on factors like the Forrest classification and ulcer location/type. For gastric outlet obstruction and perforation, the document compares non-operative and operative options and factors like vagotomy type, drainage procedures, and H. pylori status that influence choice of treatment.