Downloaded 882 times
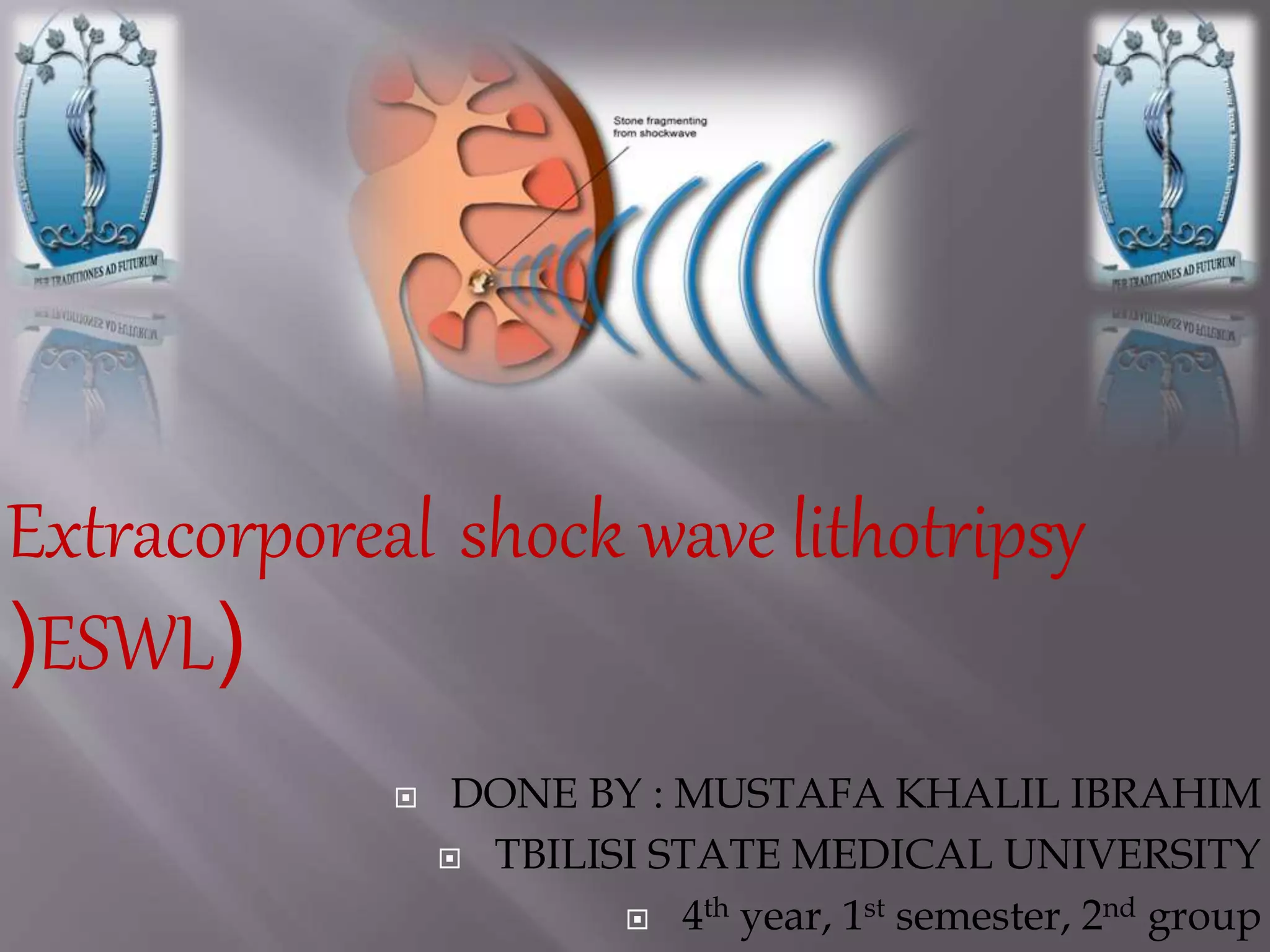









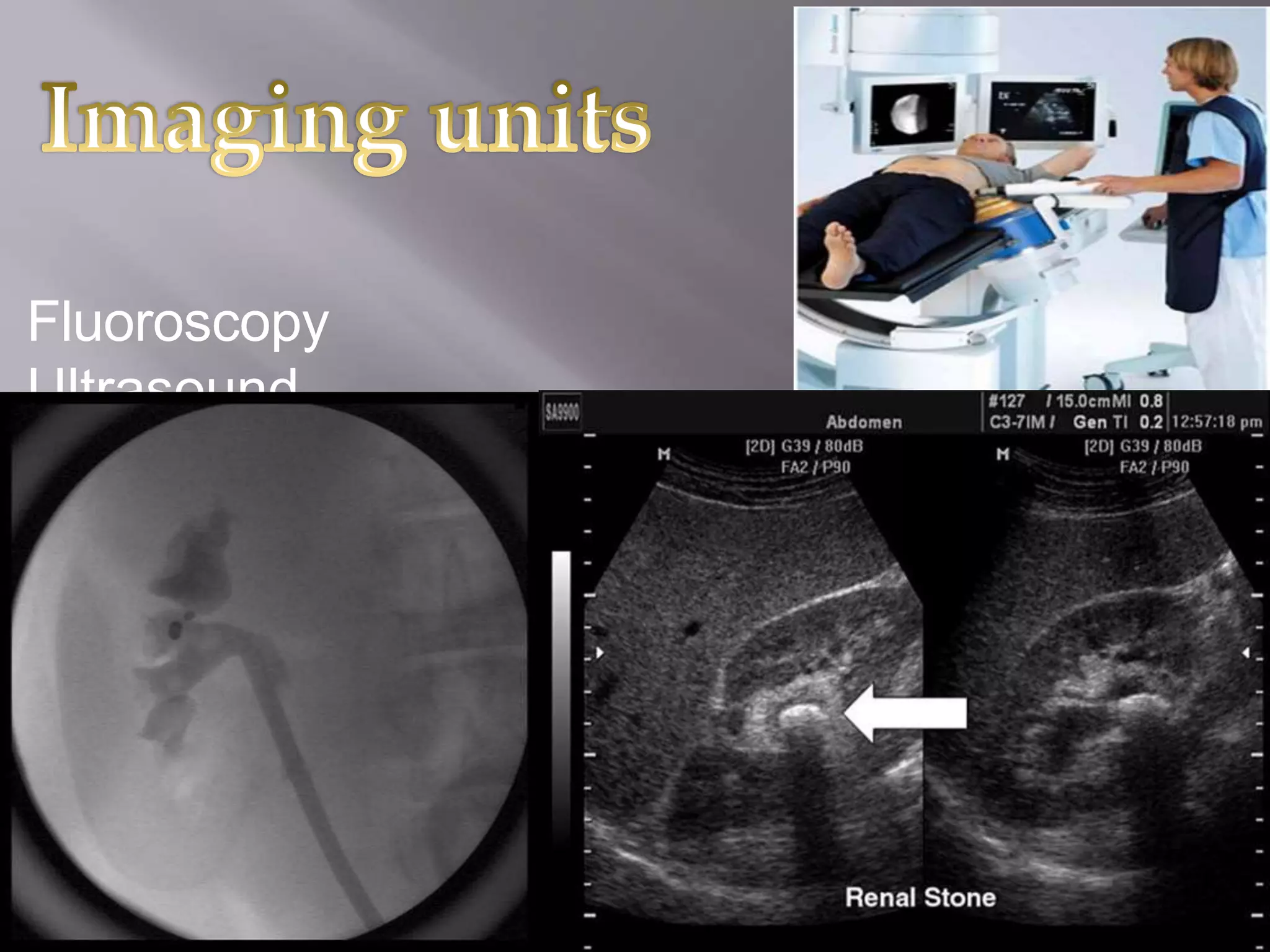



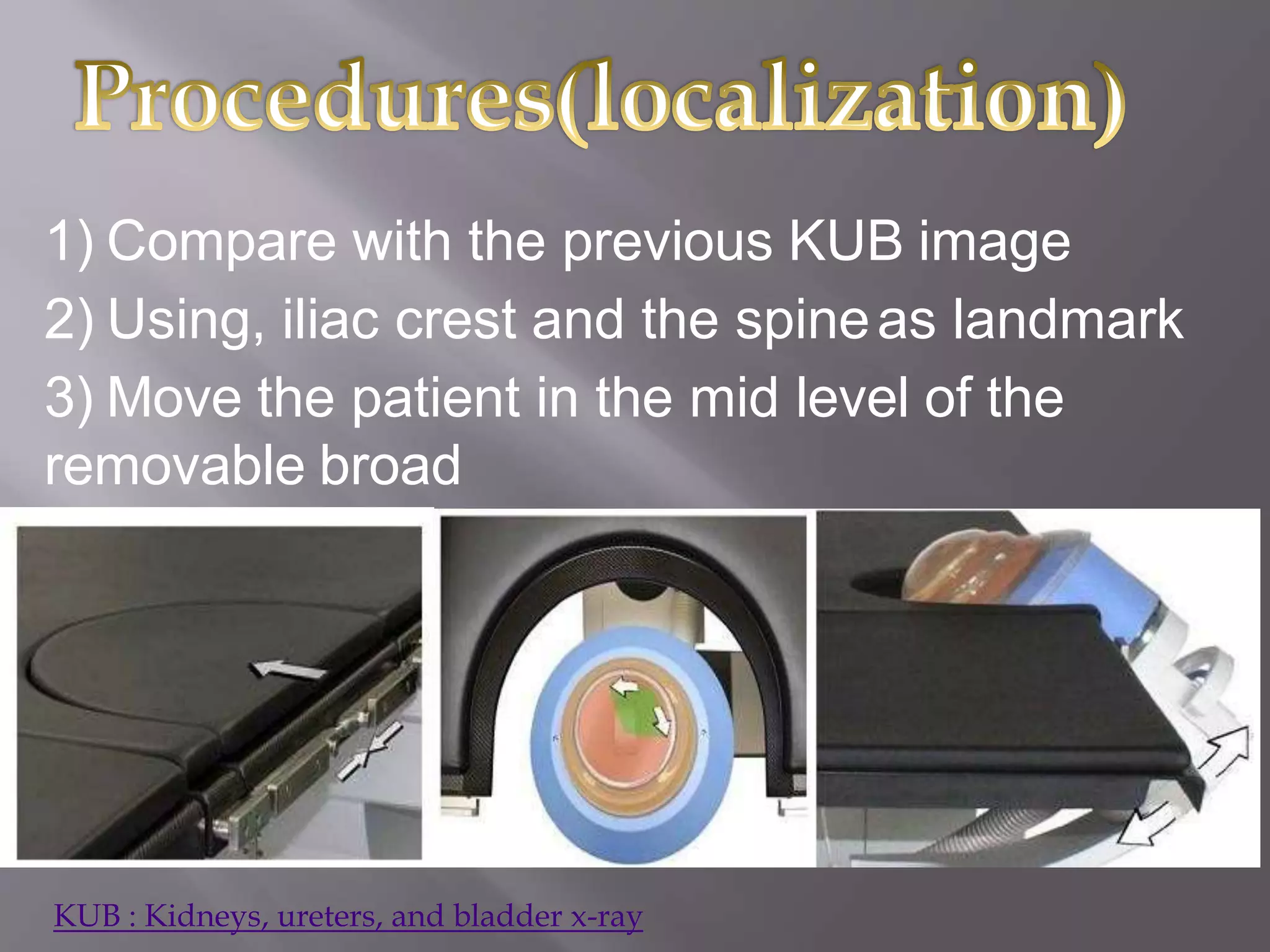





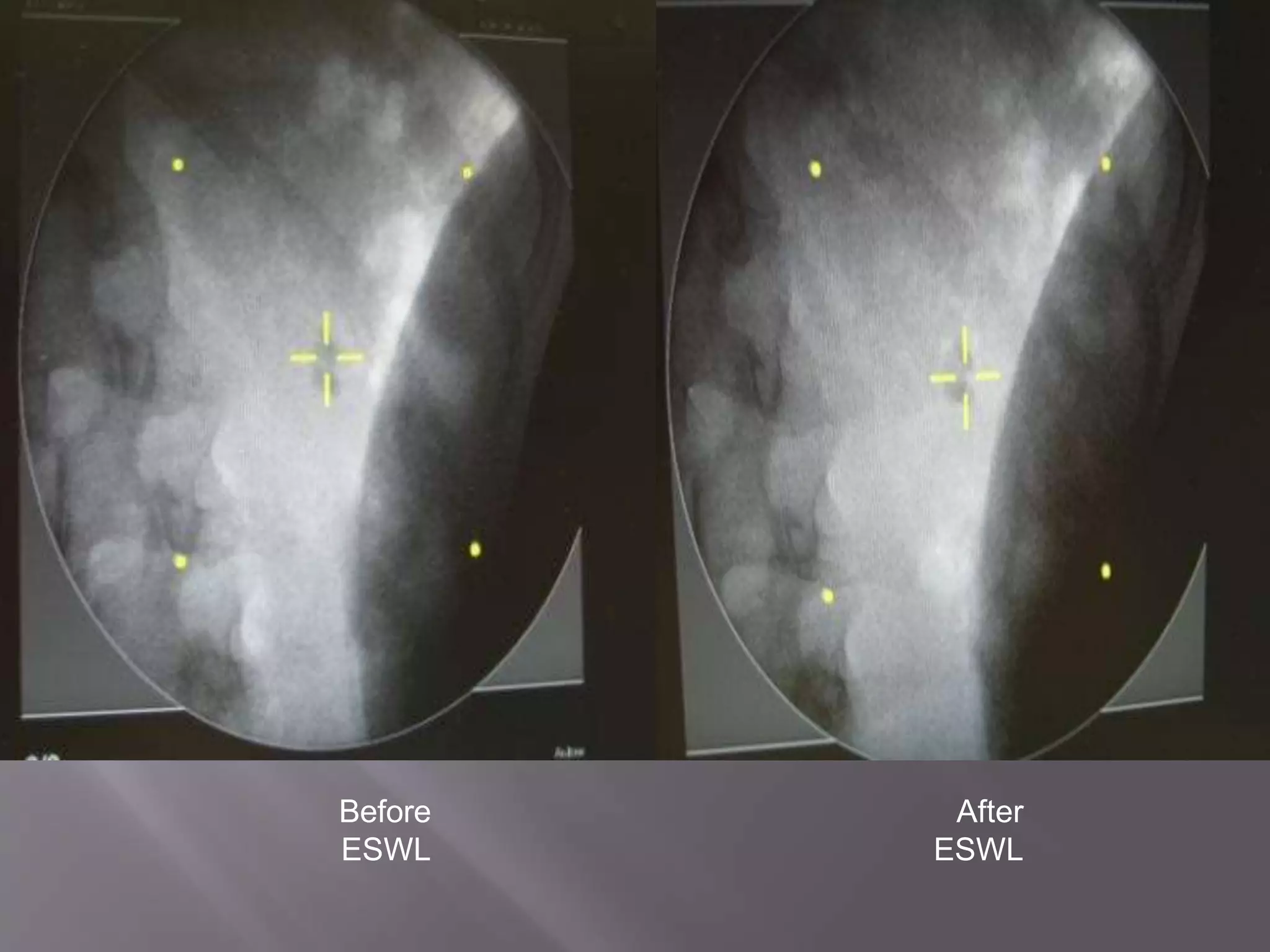







This document discusses extracorporeal shock wave lithotripsy (ESWL) for treating kidney stones, outlining the types of stones and symptoms, as well as the procedure's mechanism and equipment used. It also covers patient preparation, treatment parameters, monitoring, and potential risks and advantages of ESWL. Various sources are cited for further reading on the topic and procedural guidelines.






























































































