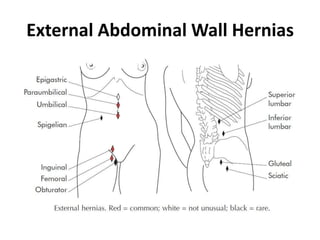
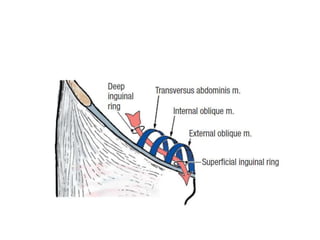
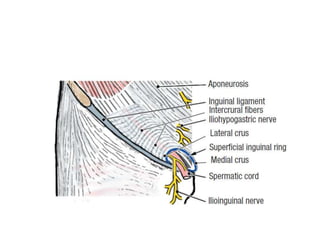
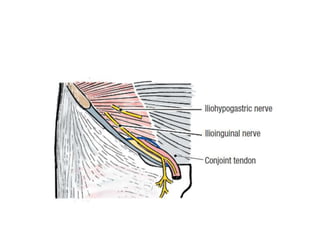
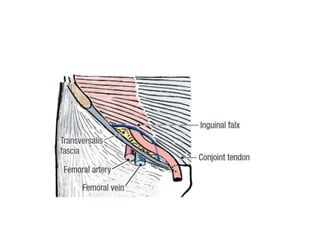
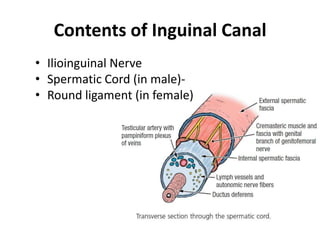
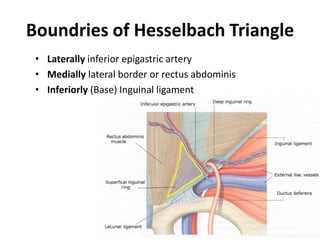
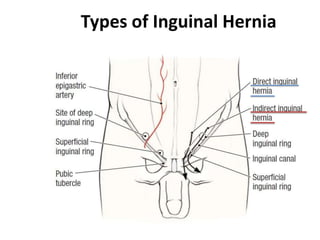
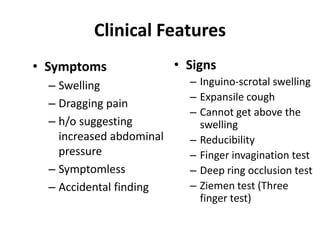
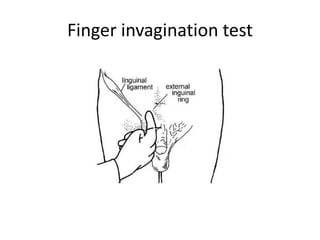
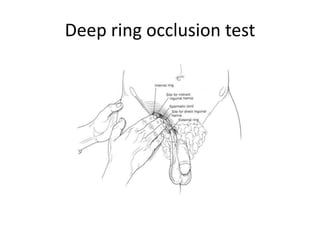
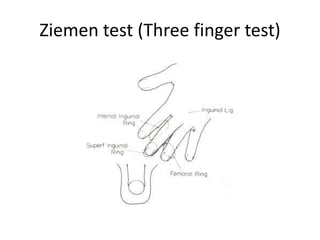
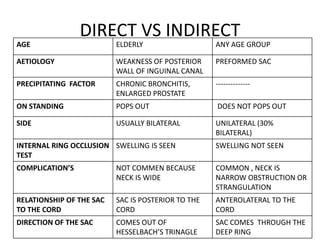
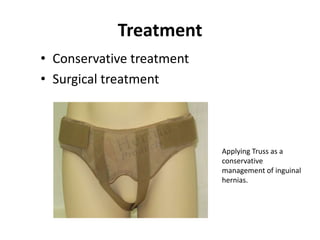
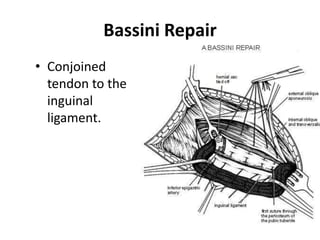
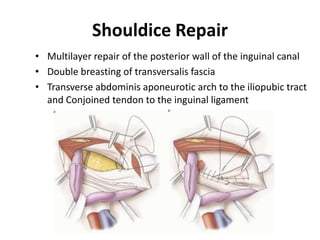
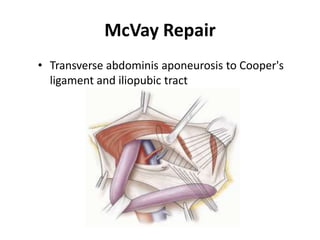
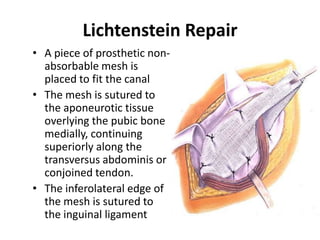
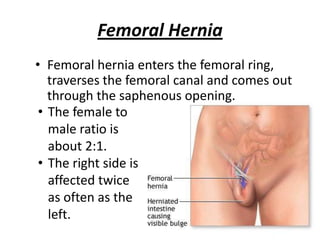
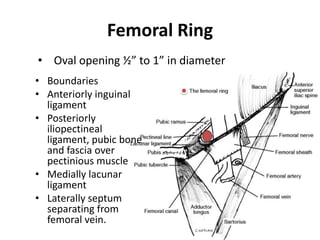
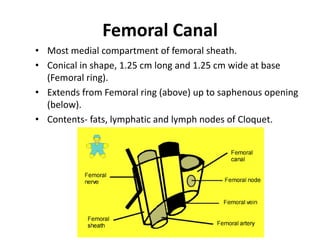
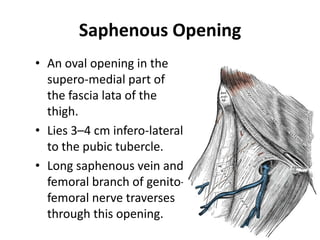
This document provides an overview of abdominal wall hernias, including definitions, types, etiologies, anatomy, clinical features, and treatments. It describes the main types of groin hernias such as indirect, direct, and femoral hernias. It discusses the composition of hernias and provides classifications. For groin hernias specifically, it outlines the anatomy of the inguinal canal and contents, compares indirect and direct hernias, and describes surgical repair techniques like Bassini, Shouldice, and Lichtenstein. Femoral hernias are also summarized, including the anatomy of the femoral ring and canal.