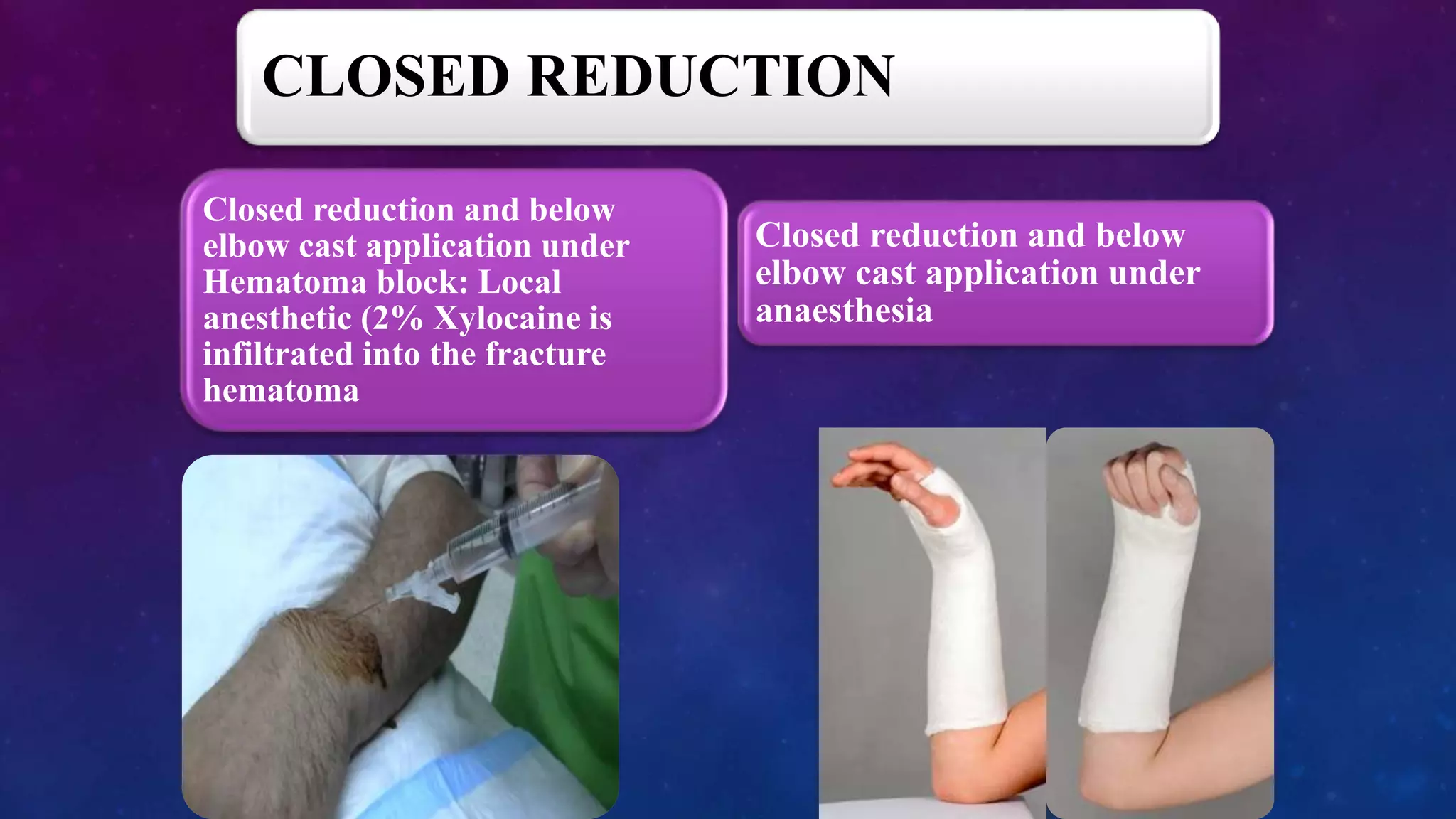
traction on fingers
Surgeon: manipulates distal
fragment into position
Cast immobilization for 6-8
weeks
Follow up X-rays at 2 weeks, 6
weeks
Check for maintenance of
reduction
Gradual mobilization after cast
removal
Physiotherapy
Return to activities in 6-8 weeks
Complications: malunion, non-
union, reflex sympathetic
dystrophy
Indications for surgery:
- Irreducible fracture
- Significant displacement after
reduction
- Open fracture
- Associated injuries of distal
radioulnar joint
Surgical options:
- Percutaneous pinning
- External fixation
- Open reduction and internal
fix