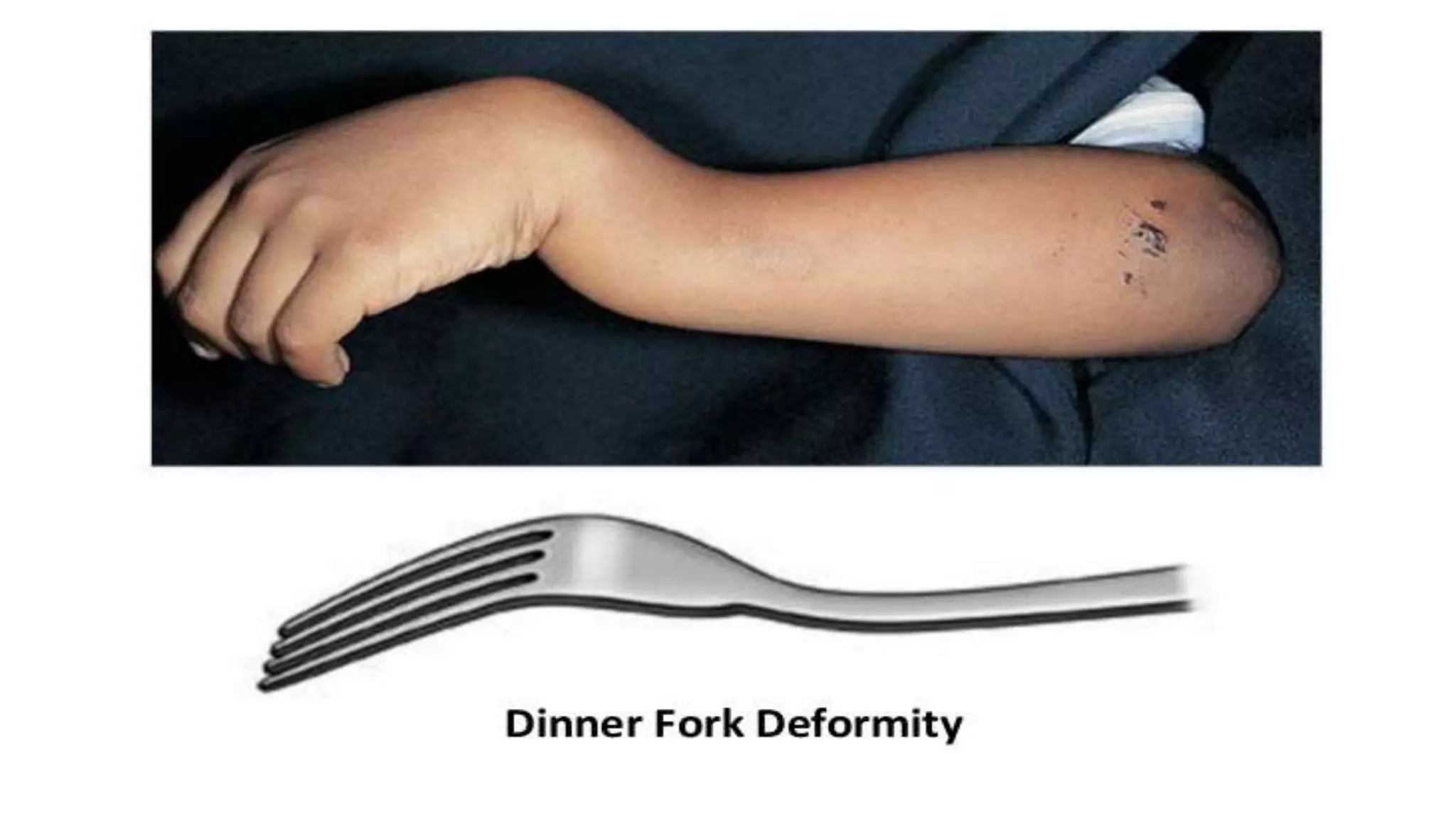
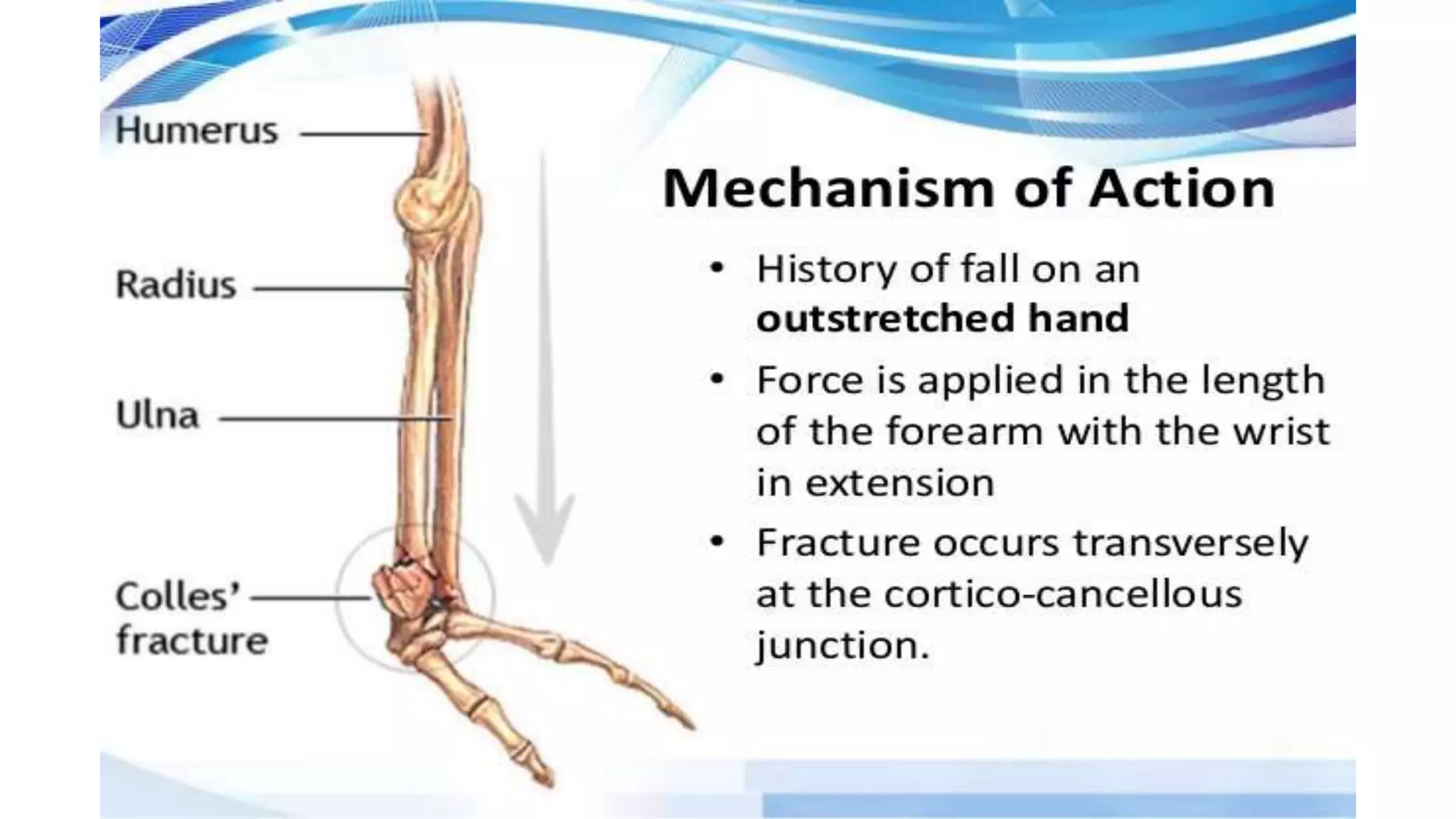
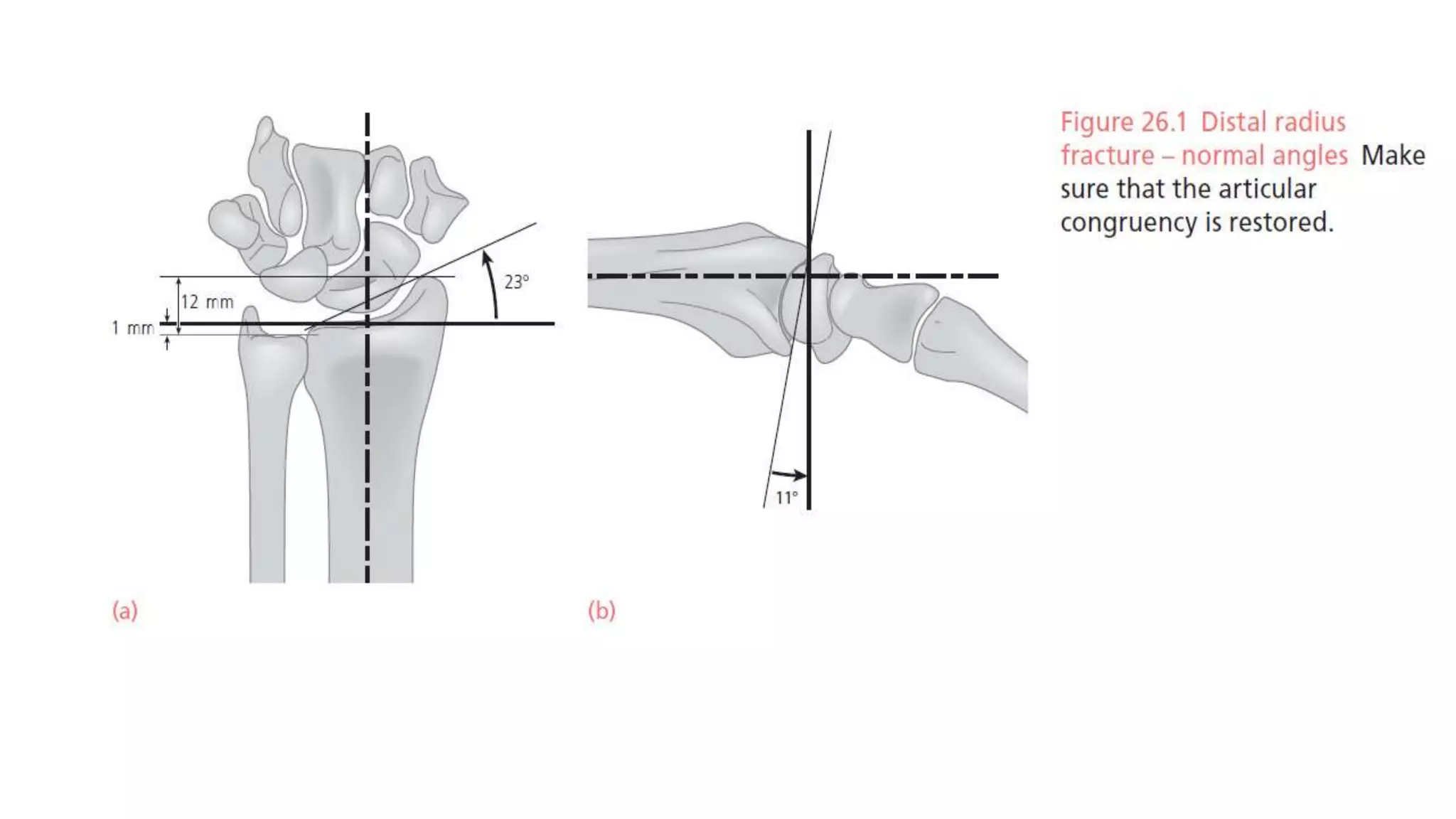
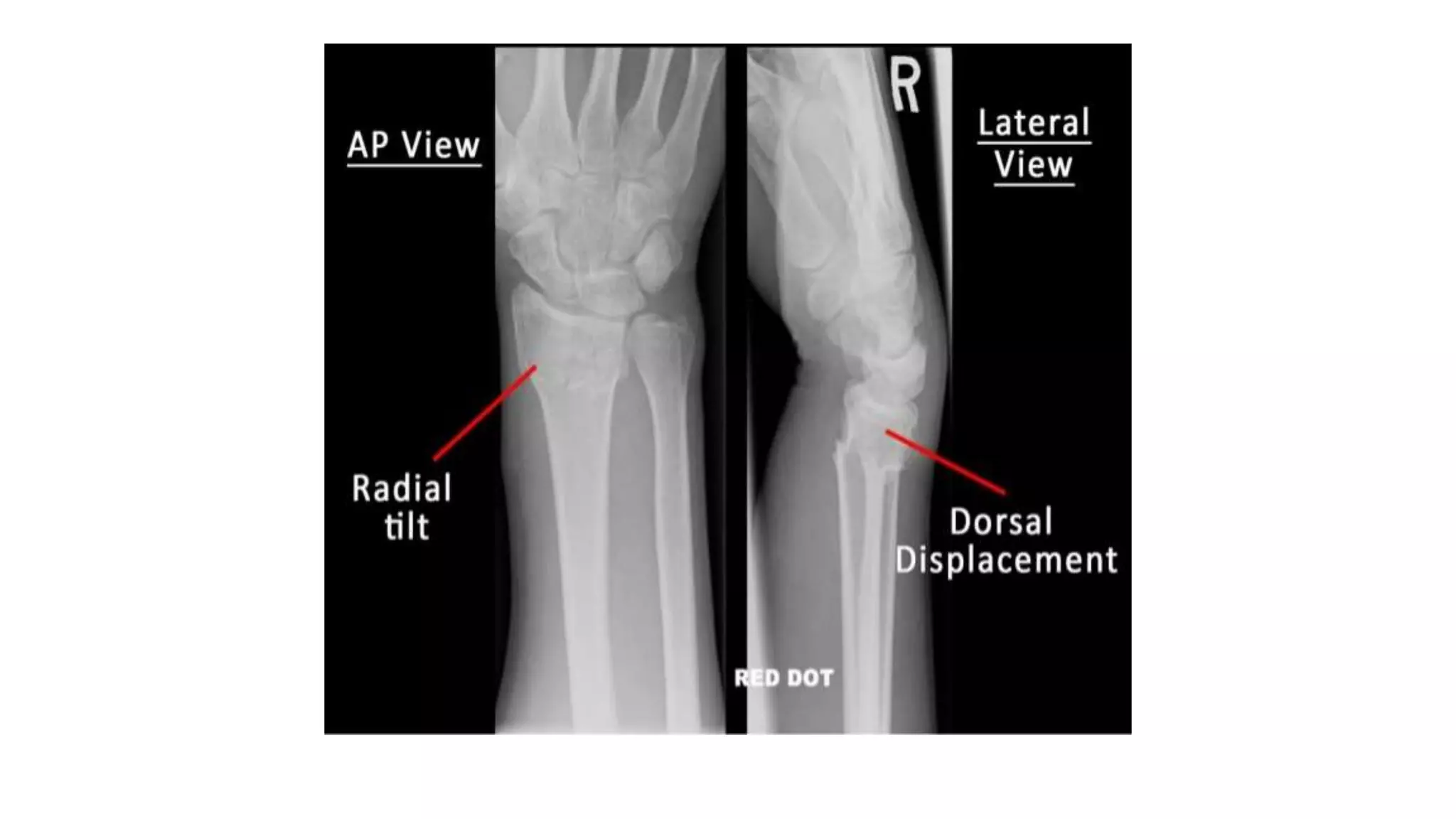
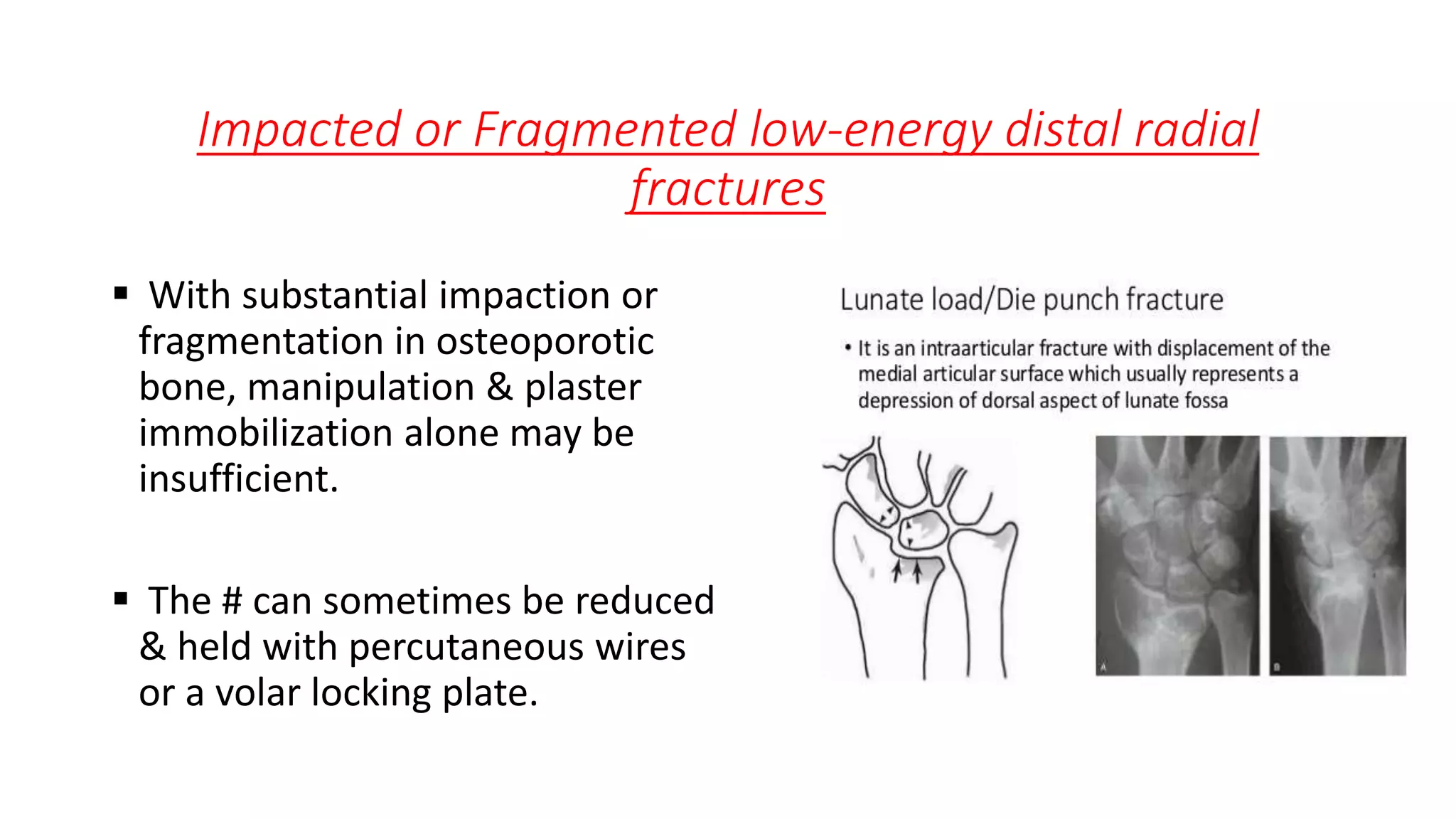
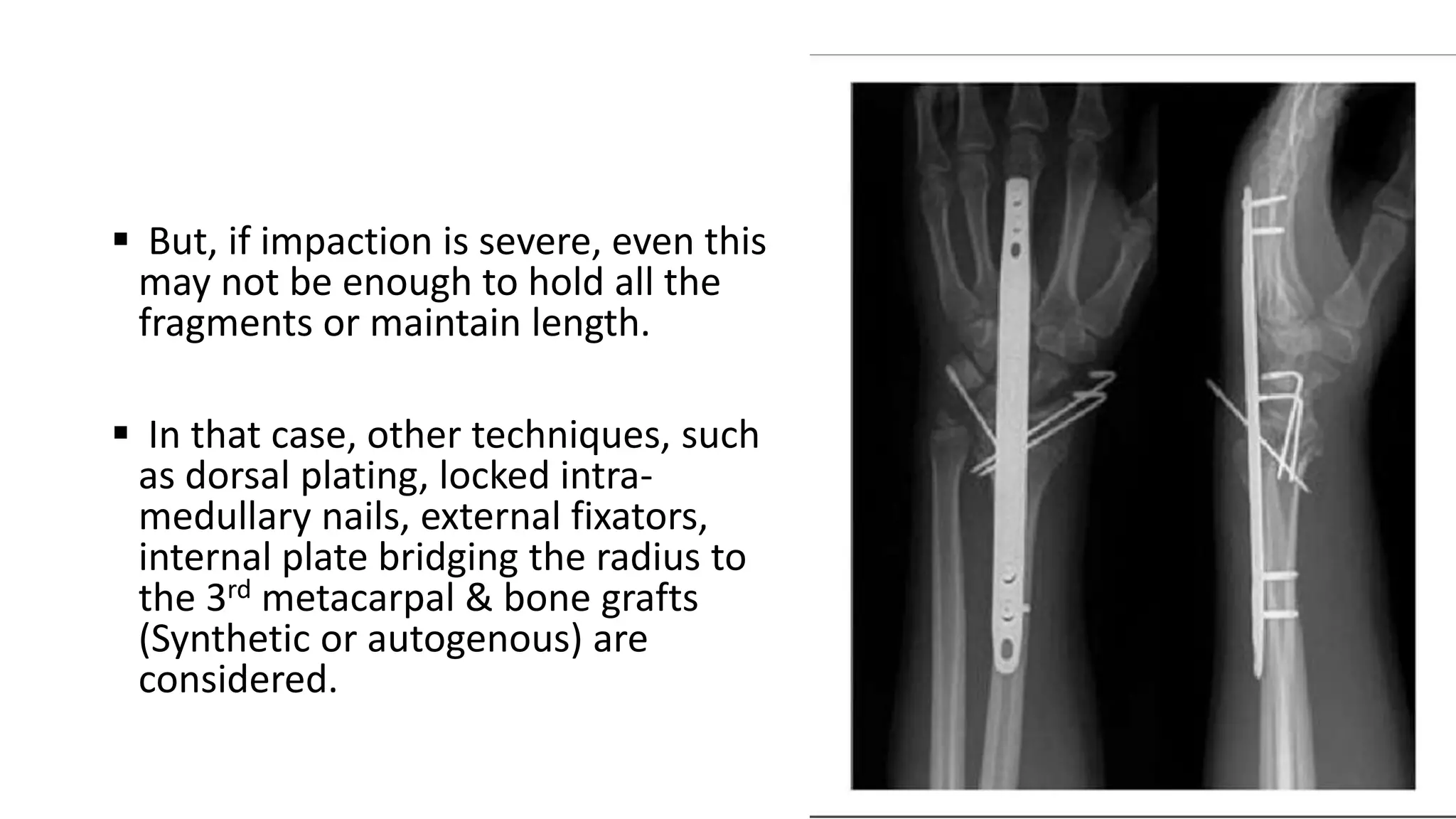
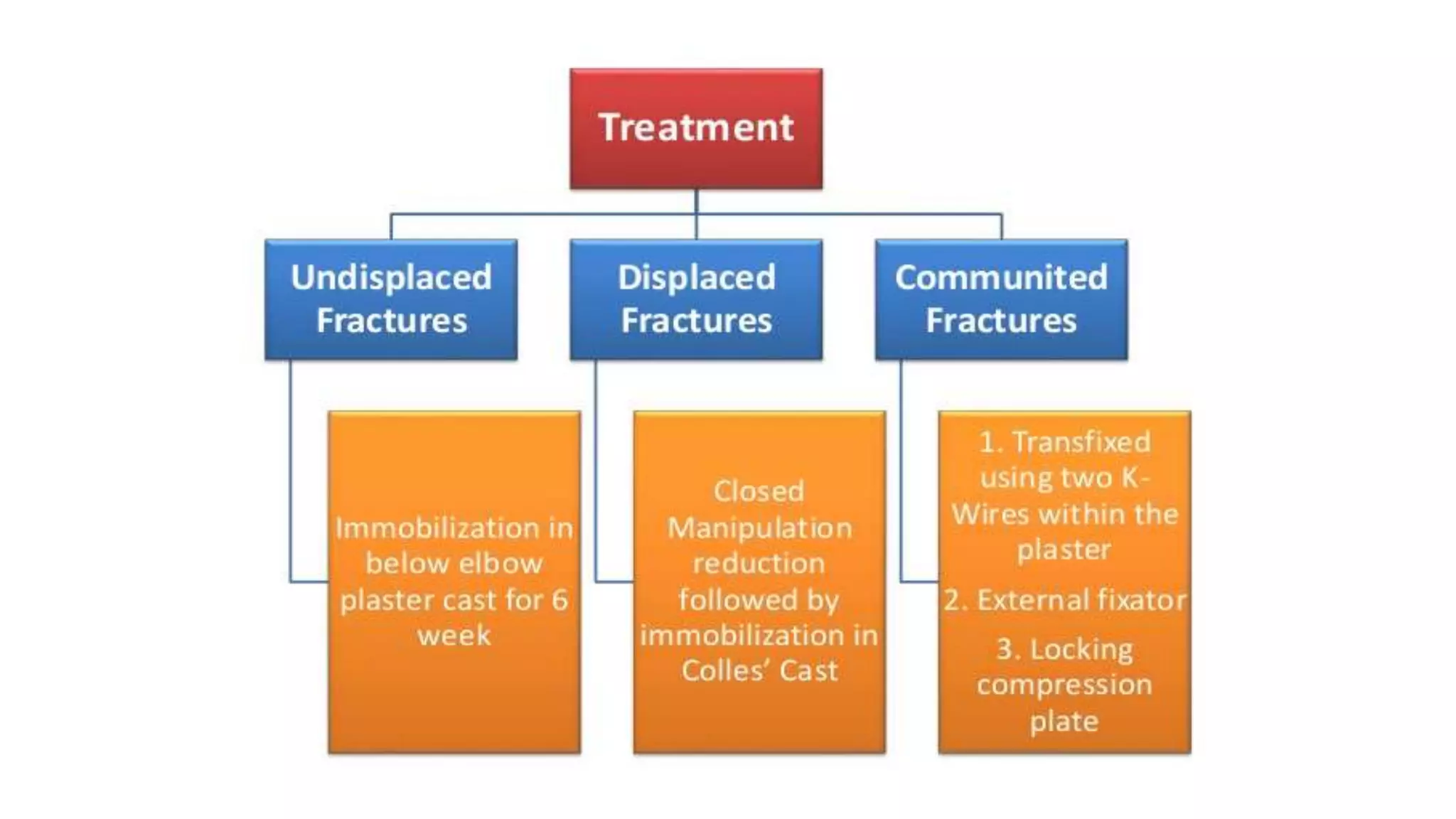
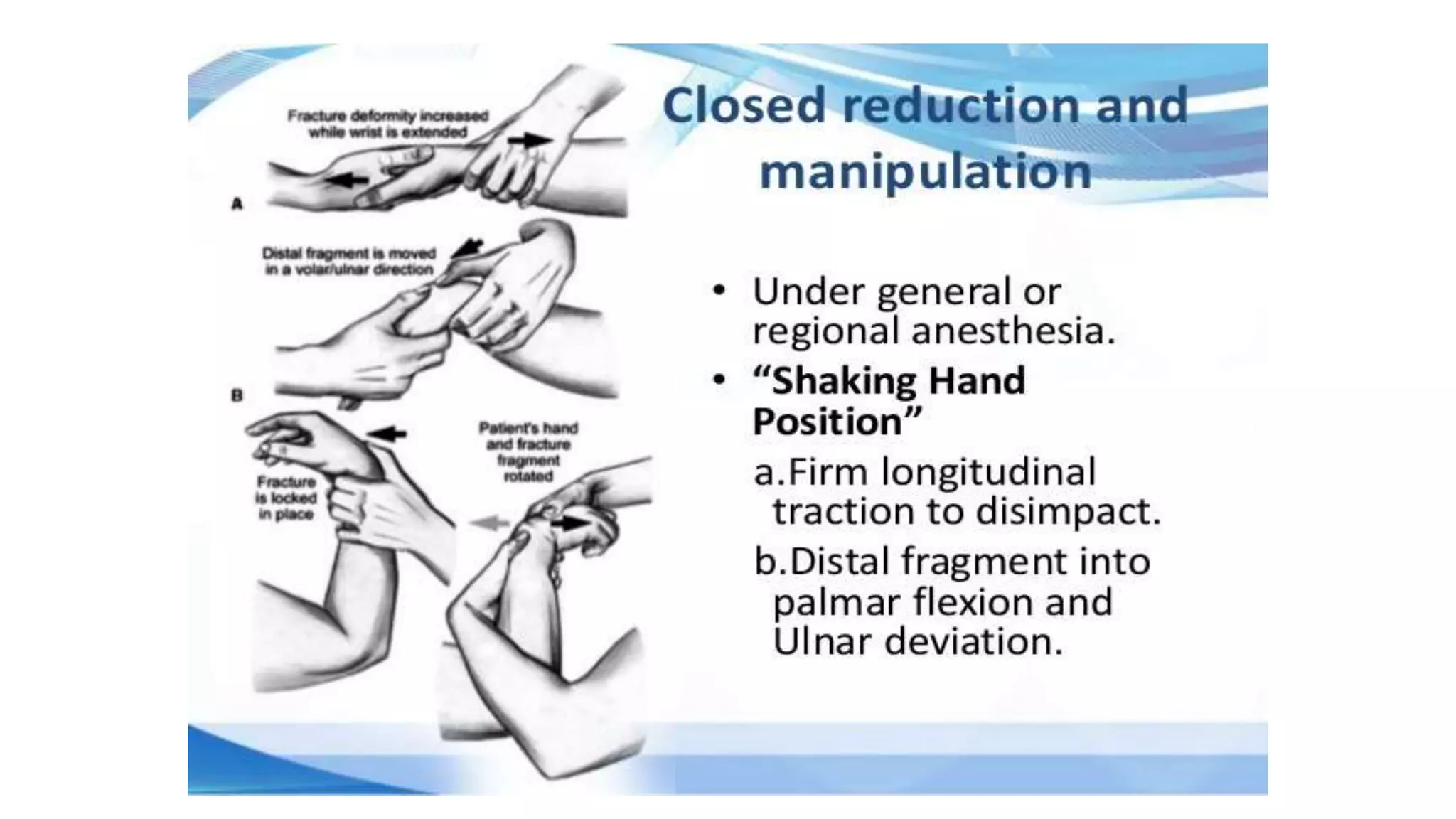
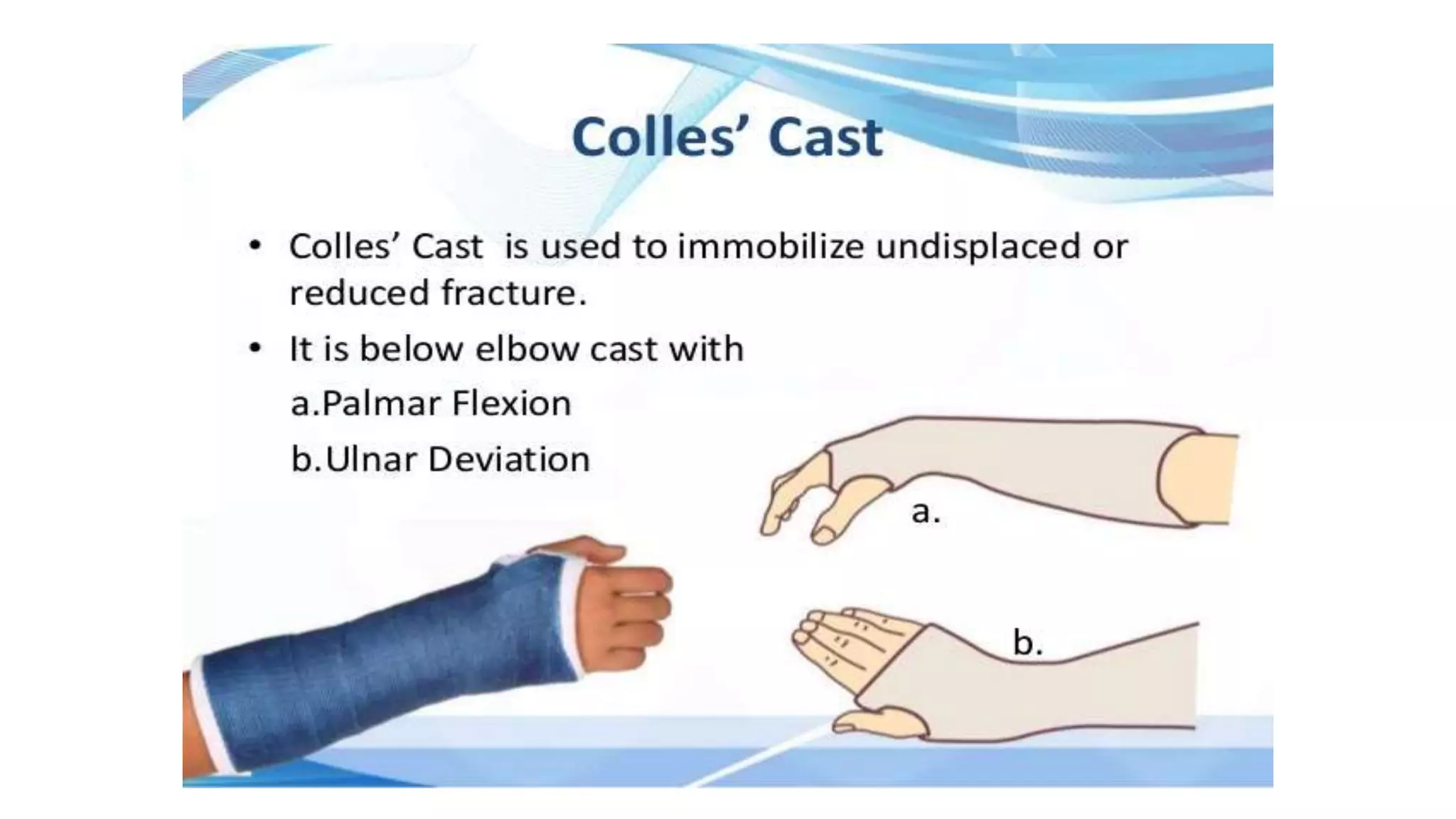
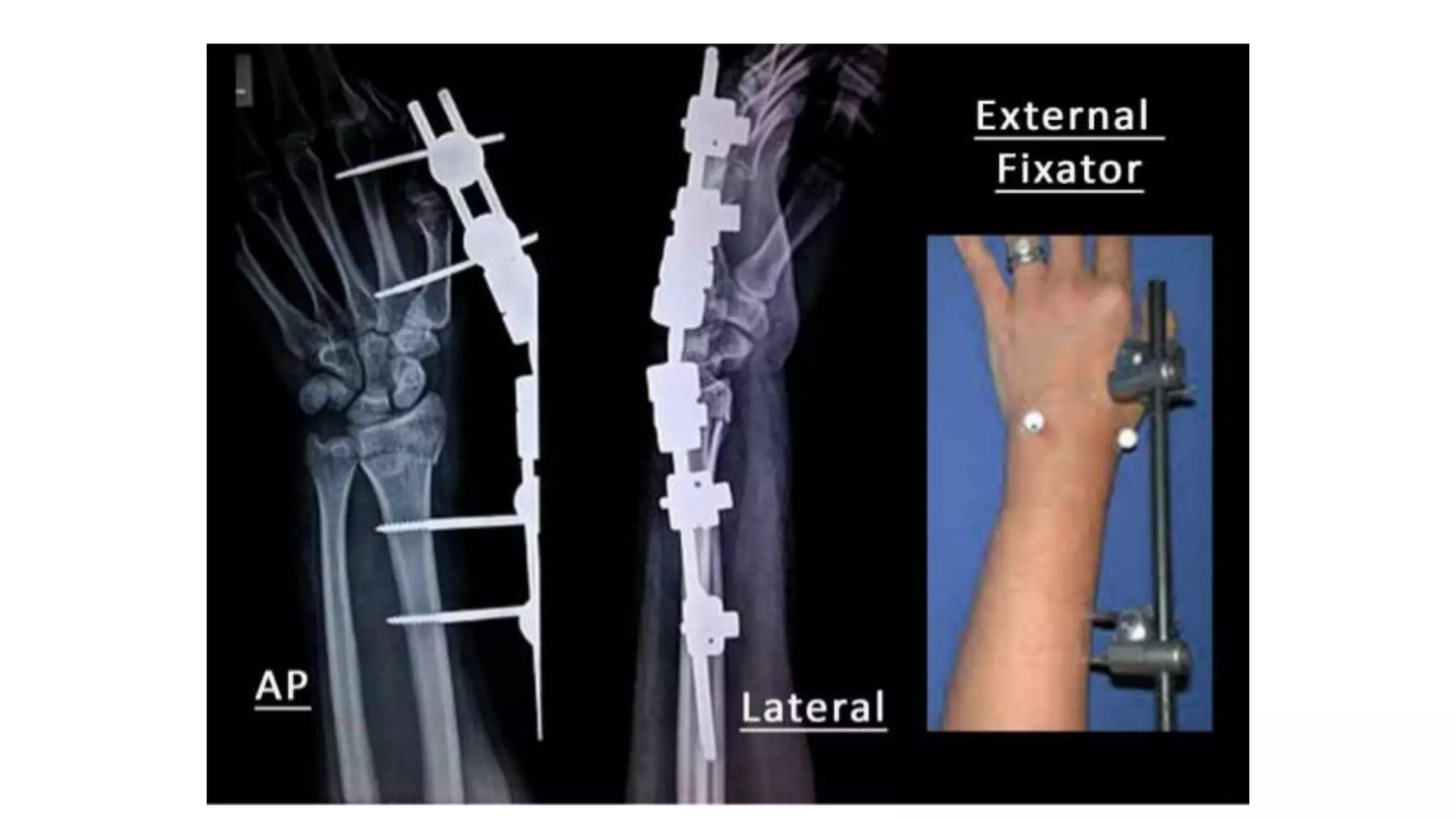
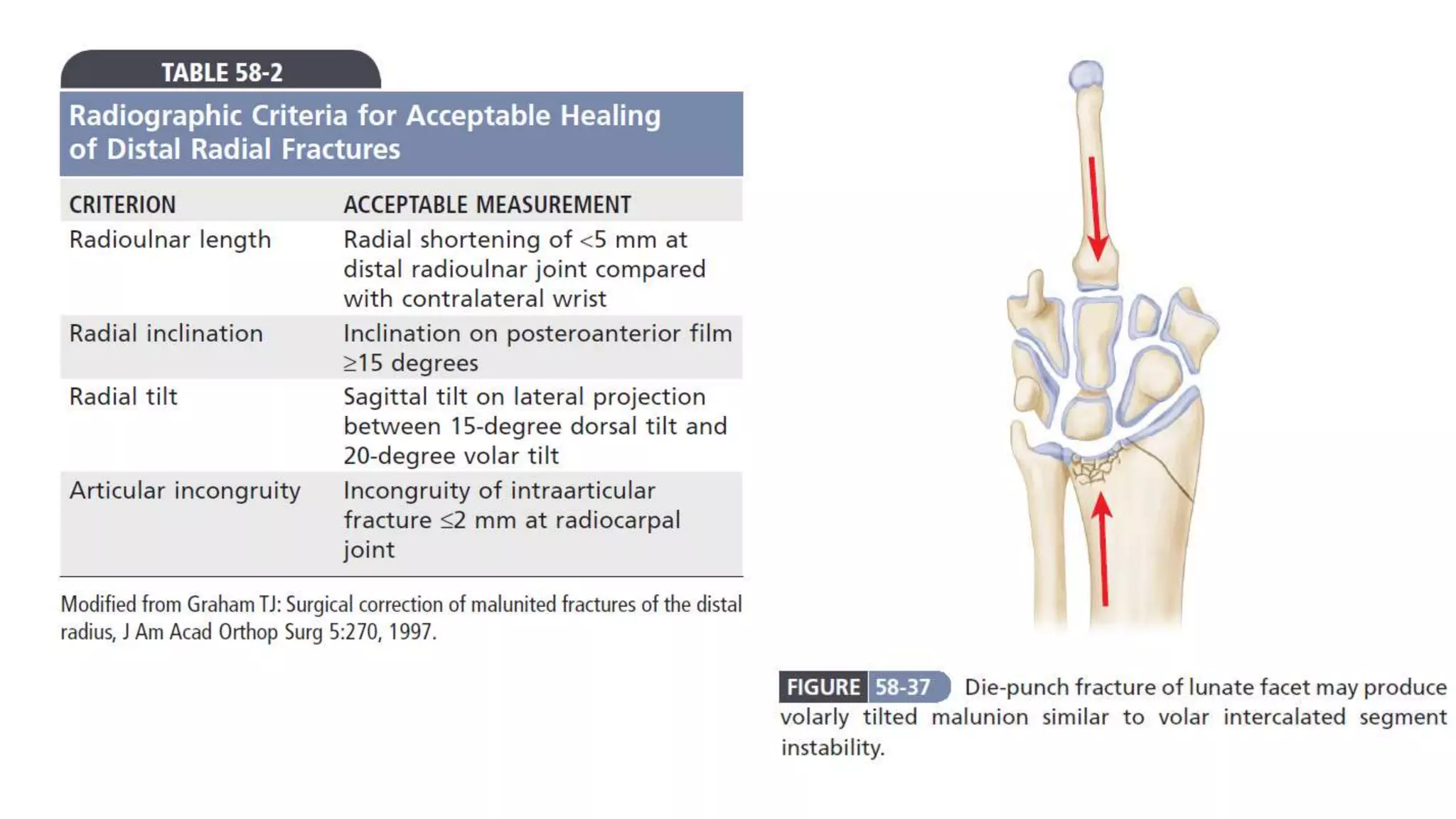
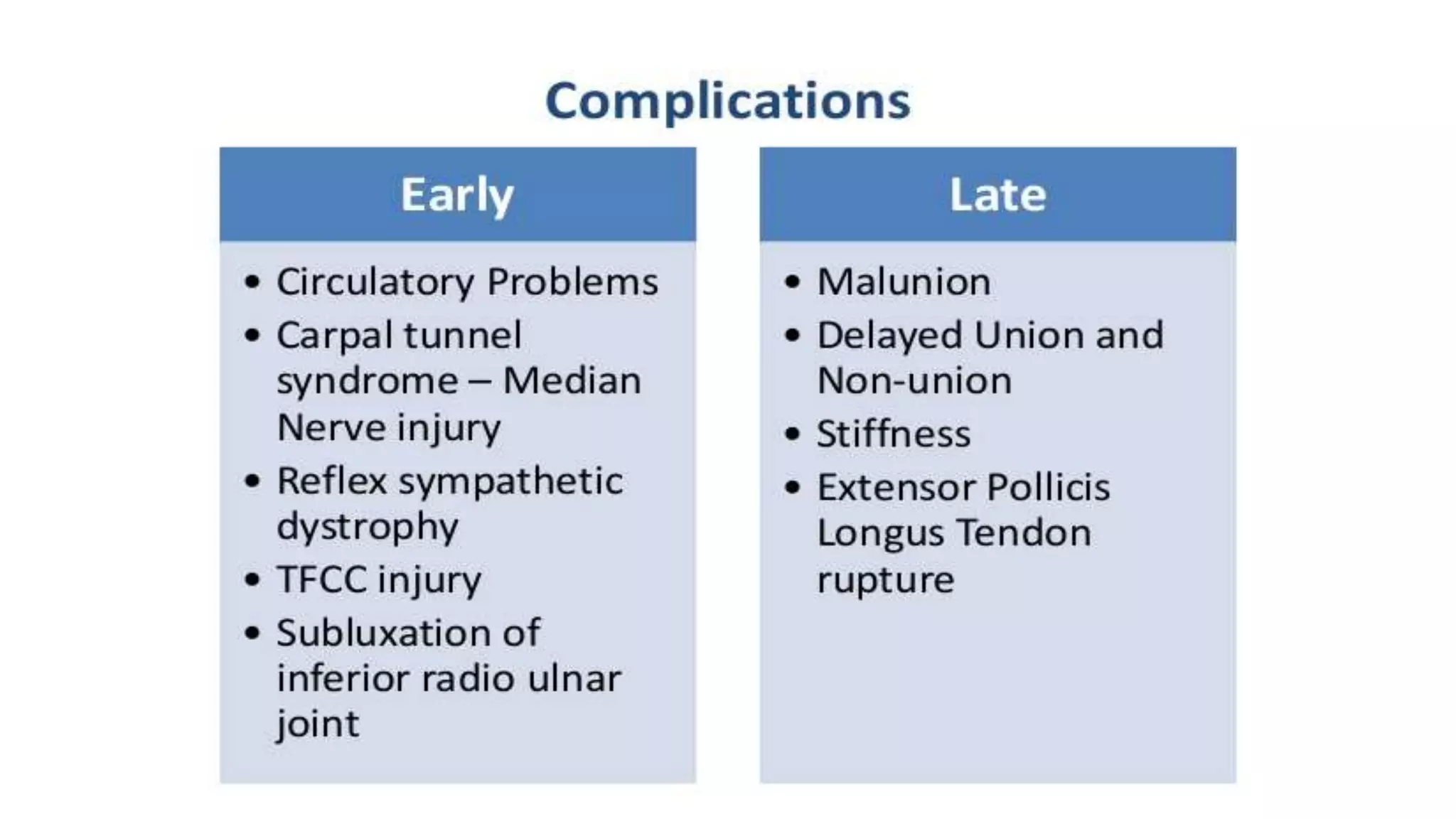
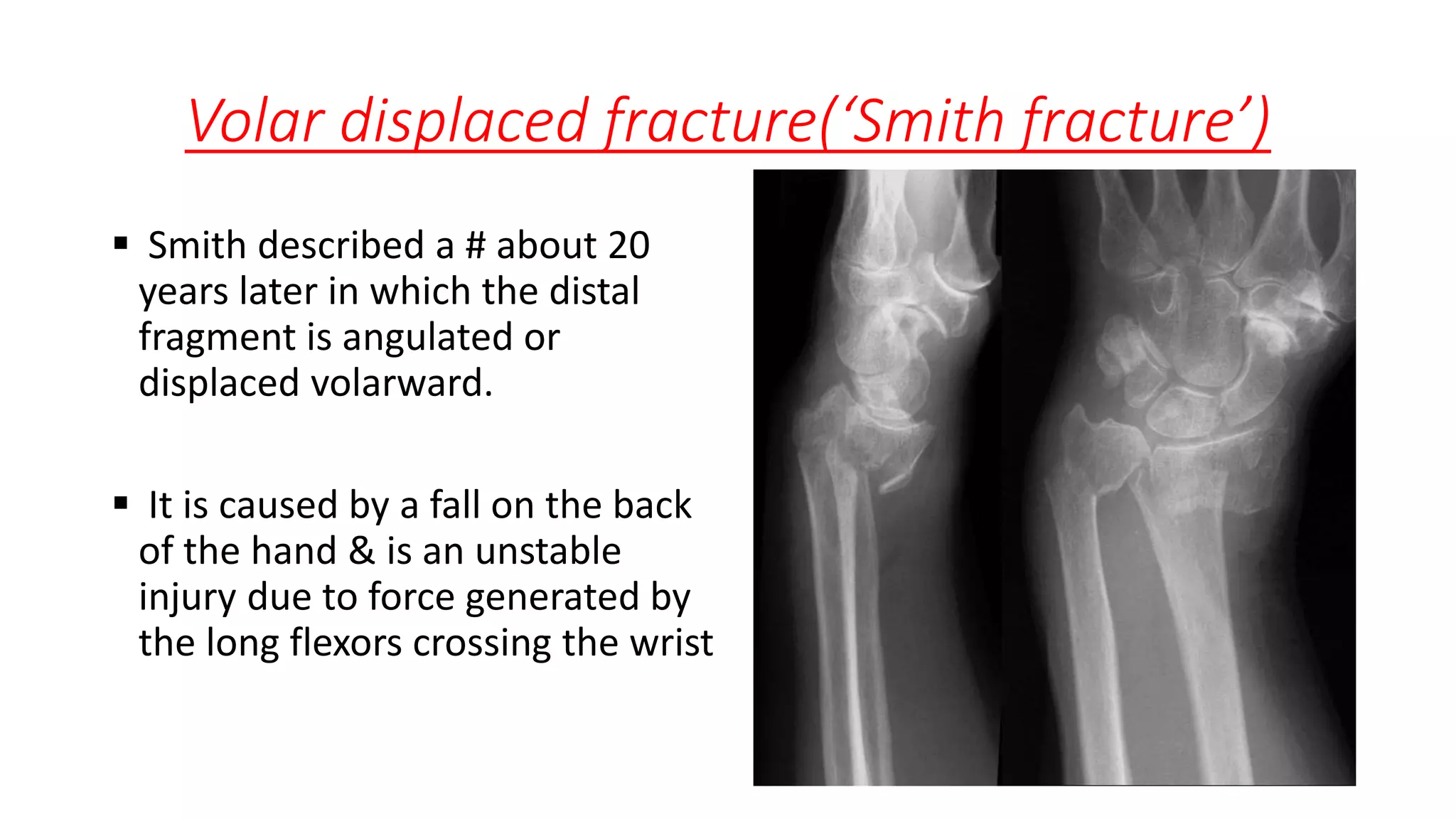
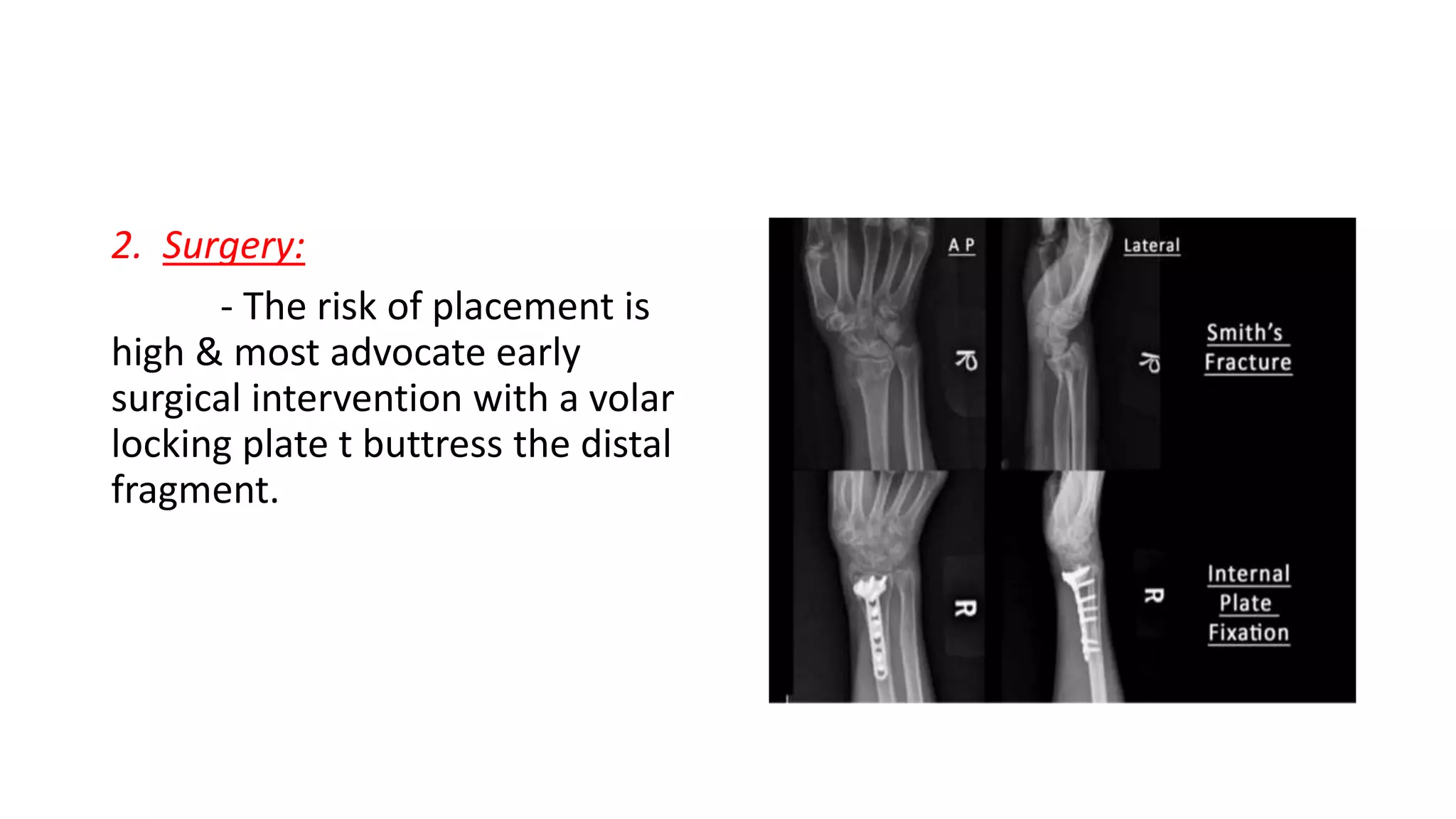
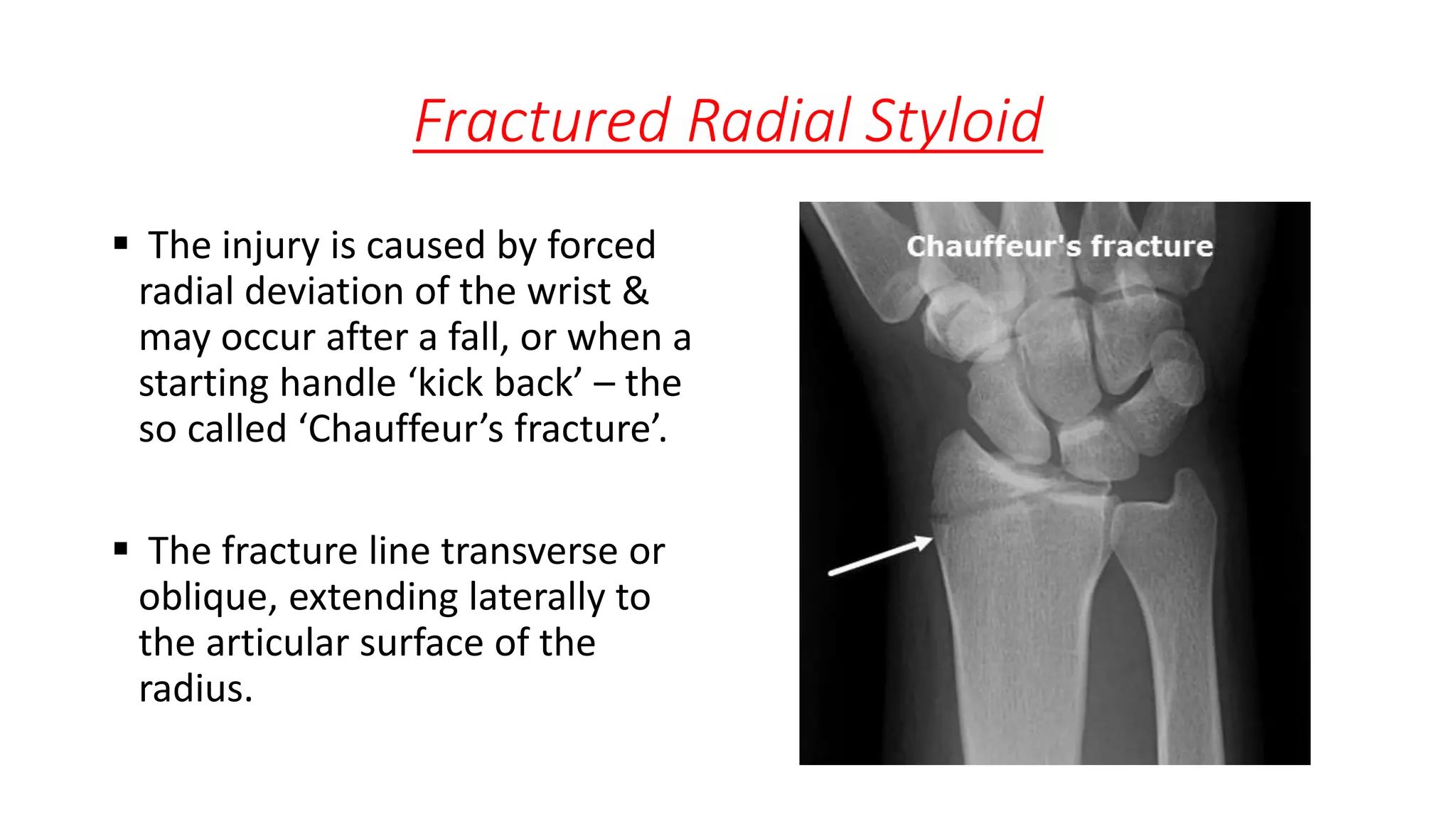
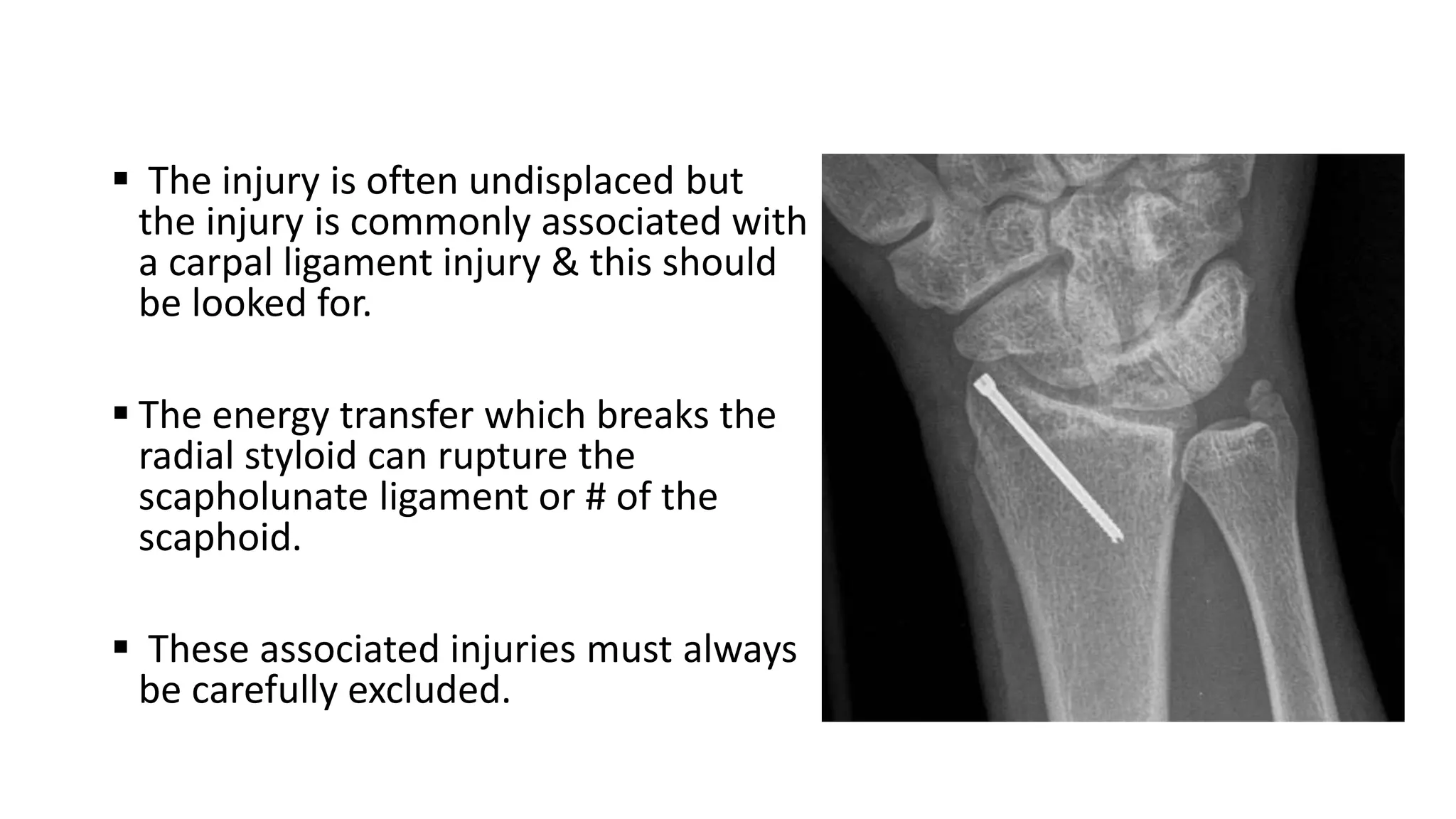
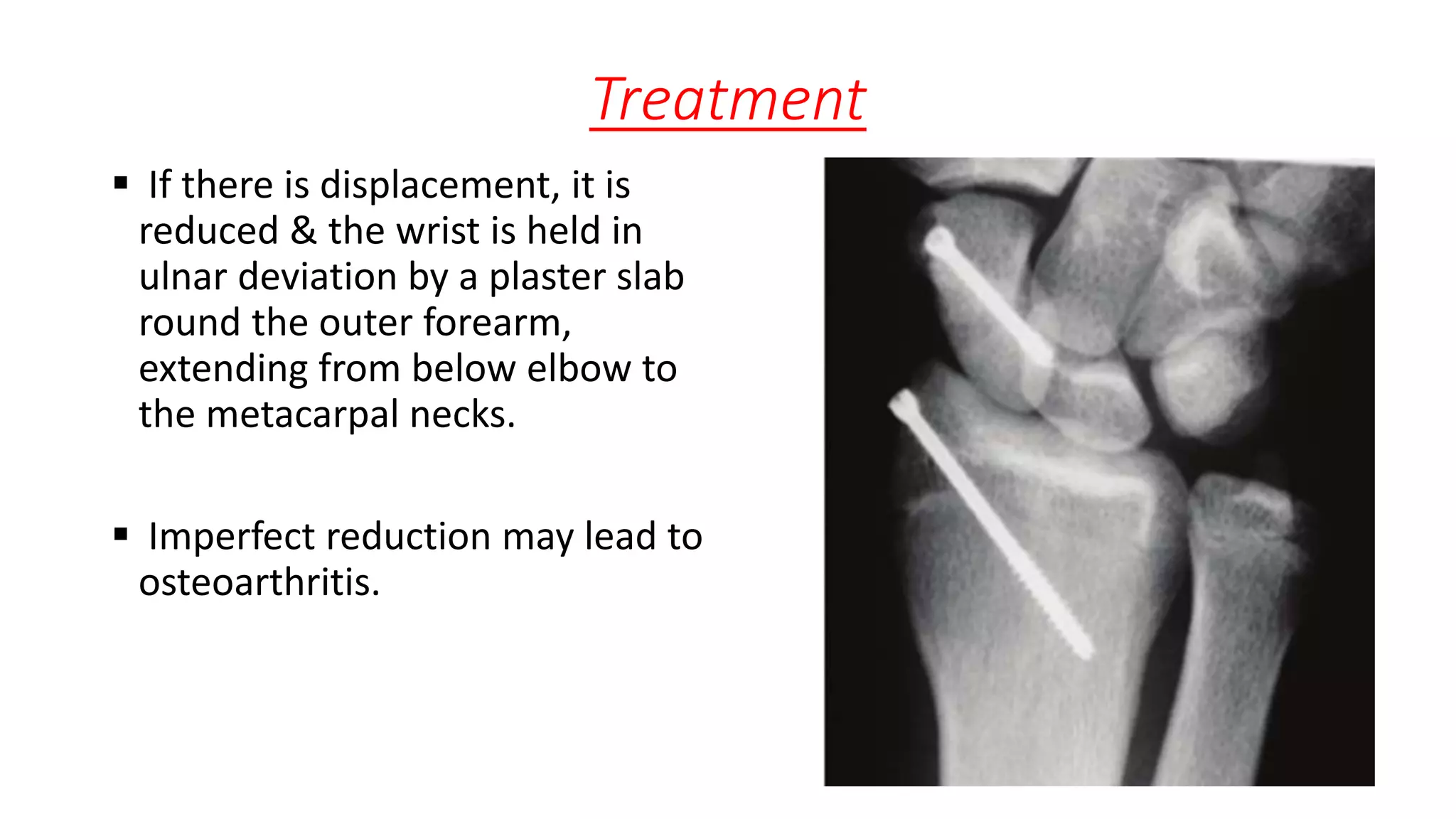
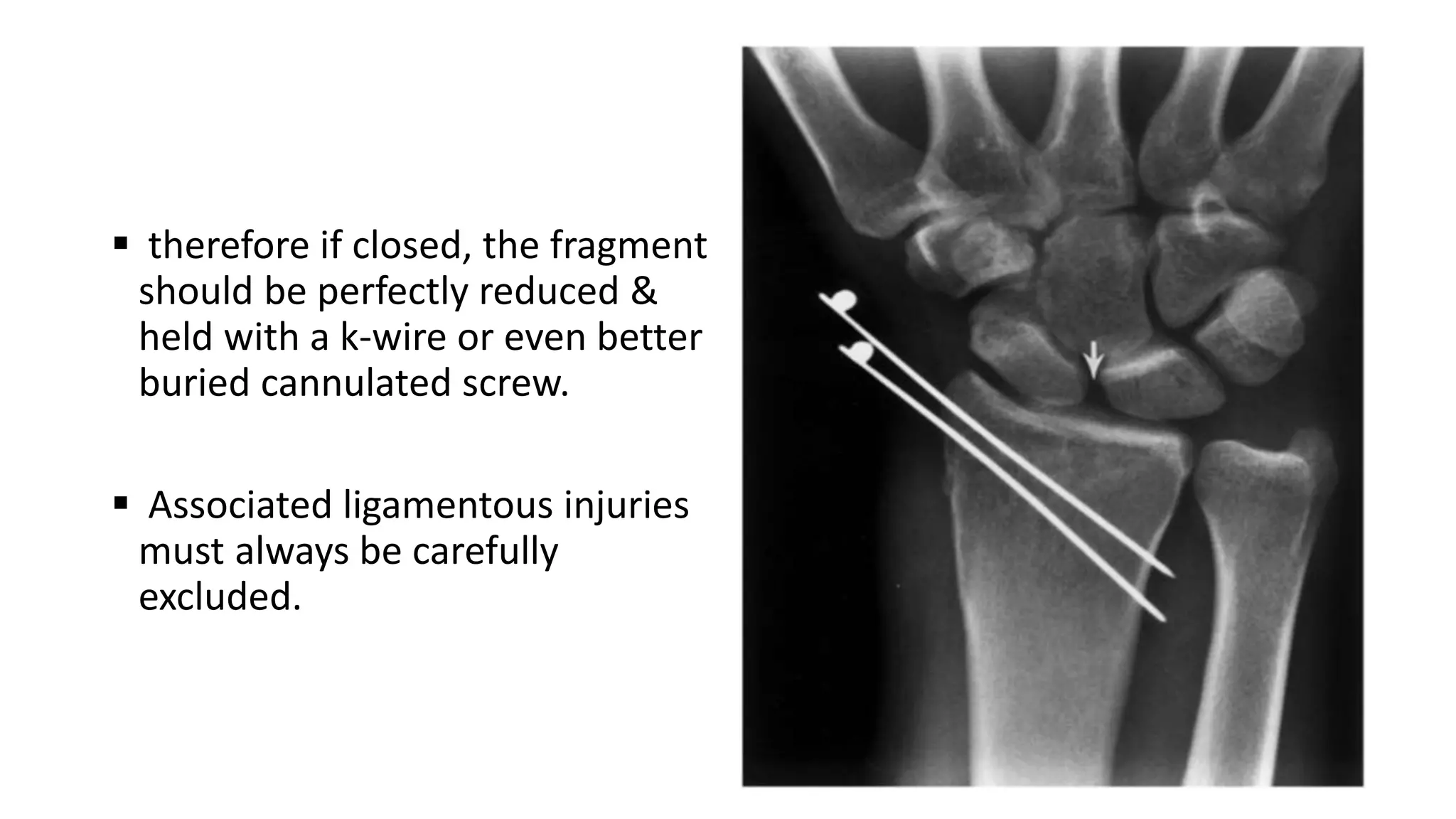
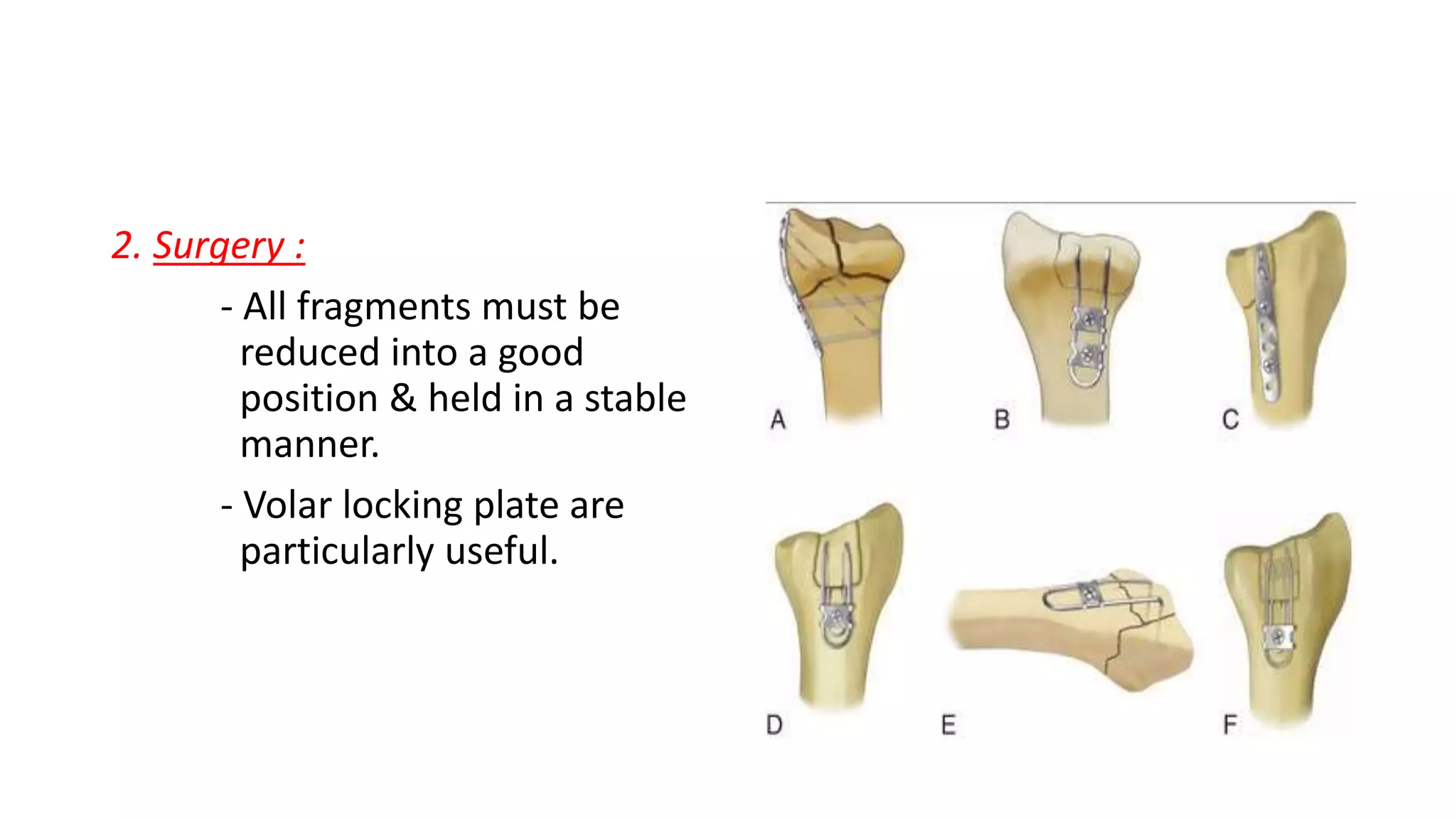
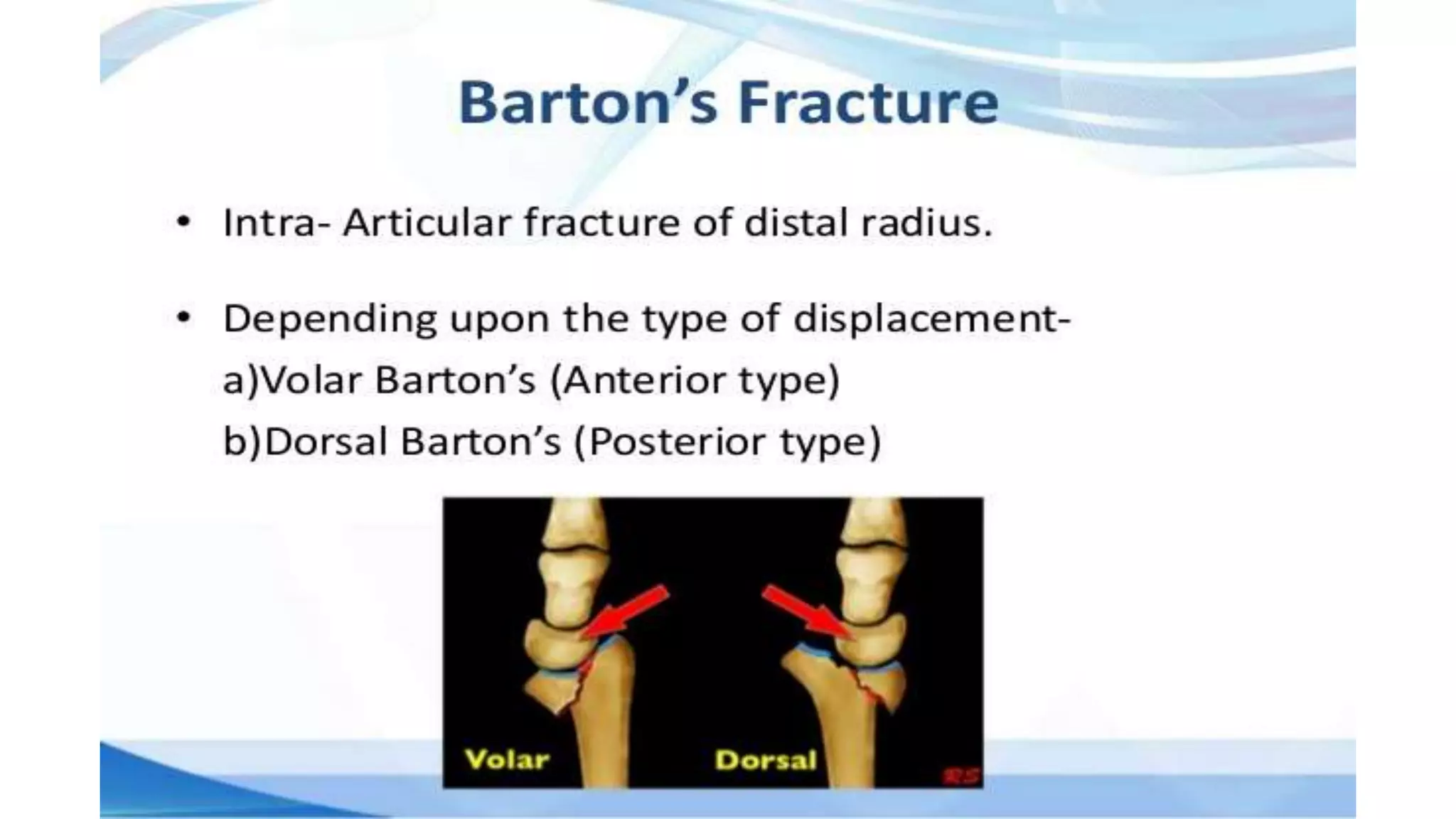
This document discusses fractures of the distal radius, including Colles' fractures (transverse fractures with dorsal displacement), Smith's fractures (volar displacement), and Barton's fractures (dorsal or volar rim avulsions). Treatment depends on the fracture type and degree of displacement/fragmentation. Displaced fractures may be reduced manually or surgically with K-wires, plates, or external fixation. Outcomes depend on restoring length, alignment, and congruity while allowing early motion. Complications include malunion, nonunion, instability, and arthritis.











































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)
























































