FOREARM FRACTURES
BESA JUSTINEJNR
4TH YEAR MEDICIAL
STUDENT
12TH
AUGUST, 2025
My qualifications; GRADE 7,9 AND 12 CERTIFICATES
CLEAR PASSES FROM 1ST
TO 3RD
YEAR
MODERATOR;DR.PACO
2.
RADIAL HEIGHT; Thisis a medical measurement of the length of the distal radius speficifically the distance between the tip of the radial
styloid and the ulnar aspect of the distal articular face.In cases of distal radial fractures restoring normal height is important because a
shortened is often a sign of an impacted fracture and is associated with poor functional outcomes , including pain and restricted
movement
HOW TO MEASURE IT;
1.Two parallel lines are drawn perpendicular to the long axis of the radius
2.One line is drawn along the distal articular surface of the radius
3. The second line is drawn at the tip of the radial styloid process
4.The distance between these two lines is the radial height
NB;NORMAL RANGE IS BETWEEN 9.9 TO 17.3mm
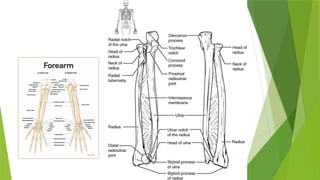
The forearm consists of the radius, ulna and hand. The anatomy of the forearm is shown below;
5.
They arefour types of forearm fractures and these are;
A.GALEAZZI FRACTURES
B.MONTEGGIA FRACTURES
C.COLLES FRACTURES
D.SMITHS FRACTURE
NB ;ALL FRACTURES ARE TREATED USING THE ATLS PROTOCOL WHICH INCLUDES;
1.PRIMARY SURVEY AND RESUSCITATION
2. AMPLE
3.SECONDARY SURVEY
4.DEFINITE FRACTURE TREATMENT
IN THIS PRESENTATION MY FOCUS IS DEFINITE FRACTURE MANAGEMENT.
6.
GALEAZZI FRACTURES; DISLOCATIONOF
THE RADIUS
MECHANSIM OF INJURY; The usual cause is a fall on an outstretched hand probably with
superimposed rotation force. It may also be caused by direct trauma or blow to the
radius.The radius fractures in the lower third shaft and the distal radio-ulna joint
incompletely dislocates or dislocates completely.
Clinical features;
A.The Galeazzi fracture is much more common than the monteggia. Always assess for
distal radio-ulnar joint disruption in all pts with radial shaft fractures
B.Prominence or tenderness over the lower end of the ulna is the stricking feature
C.Swelling and often bruising is also seen in the area off fracture
D. Pts also have wrist pain, instability or both
NB; It is important to check for ulna nerve lesion, Radial nerve ,median nerve and
anterior interosseous nerve but I will not do that since it was already discussed in
supracondylar fractures plus it is a topic on its on..
8.
MANAGEMNT
1. The goalis to restore the length of the fractured bone which is
In children closed reduction is often successful, Adults open reduction and compression plating which is ORIF is
succsseful
AN XRAY SHOULD BE TAKEN BEFORE ANY MANIPULATION OR SURGERY TO ENSURE CORRECT MX
THEY ARE THREE POSSIBILTIES;
A.The distal radio-ulnar joint is reduced and is stable; No further action is needed only arm resting for few days
then gentle active movements are advised.The radio-ulnar joint is checked clinically and radiologically after 6
wks
B.The distal radio-ulnar is reduced and unstable; Forearm should be immobilized in the position of stability
usually supination then supplemented if required by a transverse K-Wire..Forearm is splinted in an above elbow
cast for 6wks with a window on the site of K-wire
The distal radio-ulnar joint is irreducible; unsual, open reduction is needed to remove the interposed soft
tissues… The triangular fibrocartilage complex and dorsal capsule are then carefully repaired and forearm
immobilized in the supination position for 6 wks
9.
MONTEGGIA FRACTURE;DISLOCATION OF
THEULNAR
Previously this described a fracture of the shaft of the ulna associated with dislocation of the proximal
radio-ulnar joint.The radiocapitellar joint is inevitably dislocated or subluxated as well
Recently it also entails any fractures of the ulna associated with dislocation of the radio-capitellar joint.
If the ulnar shaft fracture is angulated with the apex anterior then the radial head is displaced anterior
If the ulnar shaft fracture apex is posterior the radial head dislocation is posterior
If the fracture apex is lateral then the radial head is displaced laterally.
In children the ulnar injury maybe an incomplete fracture called greenstick or plastic deformation of the
shaft
MOA;Usually the cause is the fall on the hand if at the moment of impact the body is twisting its
momentum may forceably pronate the forearm.Somtimes the causual force is hyper-extension
CLINICAL FEATURES; The ulnar deformity is usually obvious but the dislocated head of radius is masked
by swelling .A usueful clue is pain and tenderness in the lateral side of the elbow.The wrist and hand
should be eamined for signs of injury to the radial nerve
11.
TREATMENT
Restore lengthof fractured length then can the dislocated joint be fully
reduced and remain stable
In adults , the ulnar fracture must be accurately reduced with the bone
restored to full length and then fixed with plate and screws, bone grafts
maybe added for safety. The radial head usually reduces once the ulna has
been fixed but if it does not then open reduction should be done
NB;If the elbow is completely stable then flexion-extension and rotation can
be started very soon after surgery but if they is doubt then arm must be
immobilized in plaster with elbow head for 6wks
12.
COLLES FRACTURE
Thisis characterized by a transverse fracture of the radius just above the wrist with dorsal
displacement of the distal fragment.It is the most common of all fractures in older people
the high incidence being related to onset of postmenopausal osteoporosis.Thus the pt usually
an older woman who give a history of falling on an outstretched hand
MOA;Force is applied in the length of the forearm with the wrist in extension.Then bone
fractures at the cortico-cancellous junction and the distal fragment collapses into dorsal
replacement, Radial tilt and shortening
CLINICAL FEATURES; DINNER FORK DEFORMITY with prominence on the back of the wrist and
a depression in front. In pts with with less deformity there may only be local tenderness and
pain on wrist movements
XRAY;TRANSVERSE FRACTURE OF THE RADIUS AT THE CORTICO-CANCELLOUS JUNCTION ABOUT
2.5cm above the wrist through the epiphysis
14.
TREATMENT
Closed manipulationunder general anaesthesia;
1. Correct the impaction first
2. Correct the radial displacement
3. Correct proximal tilt by dorsiflexion of the wrist
4. Lock the arm towards the little finger using a slab this also appears like a
dinner fork but it is a corrected one
5. Request XRAY of the wrist to check if fracture has been reduced
6. Review after a day 6 wks
15.
SMITHS FRACTURE
Inthis injury the distal fragment is displaced anteriorly which is why it is
sometimes called reverse colles.It is caused by a fall on the back of the hand
CLINICAL FEATURES;HX of trauma injury
NO DINNER FORK DEFORMITY INSTEAD A GARDEN SPADE DEFORMITY IS SEEN
XRAY;fracture through the distal metaphysis .
TREATMENT;
1. Reduced by traction, supination and extension of the wrist and forearm is
immobilized in a cast for 6 wks
2. XRAY should be taken at 7-10days to ensure the fracture has not slipped
unstable fractures should be fixed with percutaneous wires or a plate









![FOREARM_FRACTURES[1].pptx and management](https://image.slidesharecdn.com/forearmfractures1-250813120934-75e3f6d7/85/FOREARM_FRACTURES-1-pptx-and-management-16-320.jpg)
![FOREARM_FRACTURES[1].pptx and management](https://image.slidesharecdn.com/forearmfractures1-250813120934-75e3f6d7/85/FOREARM_FRACTURES-1-pptx-and-management-17-320.jpg)









































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





