Downloaded 2,235 times







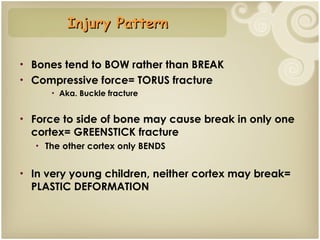























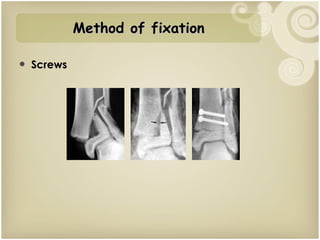
















Prof. Muhammad Shahiduzzaman discusses fractures in pediatric patients. He notes that 60% of the population in Bangladesh is under 20 years old, and fractures account for 15% of injuries in children. Fracture patterns differ from adults due to children having stronger ligaments, more cartilage, and growth plates that allow for remodeling. Common fractures include buckle fractures, greenstick fractures, and Salter-Harris fractures of the physis. Treatment depends on the fracture type but often involves closed reduction and casting, with surgery reserved for more complex cases. Children generally heal faster than adults from fractures.