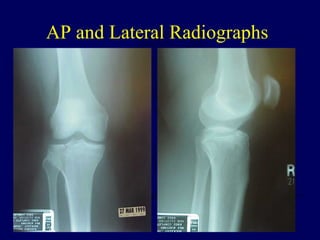
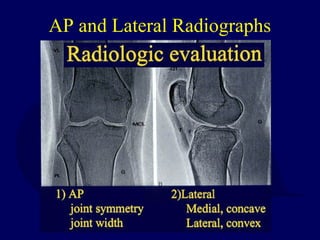
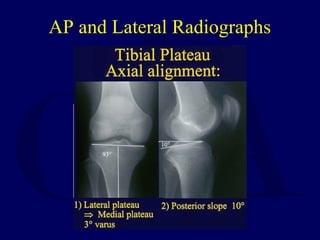
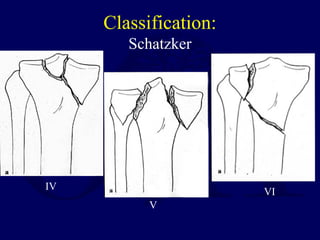
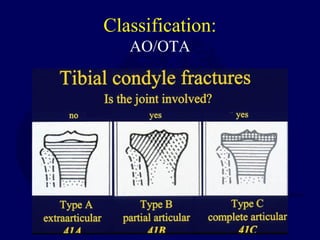
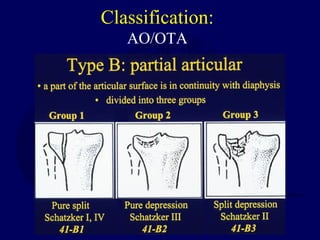
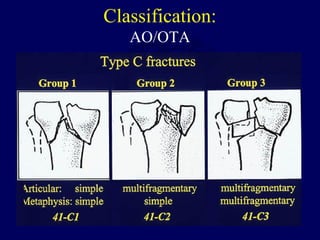
1) Fractures of the tibial plateau can be complex injuries involving both bone and soft tissues. Accurate reduction of the articular surface is important but other factors like alignment, ligament stability, and meniscal integrity also influence outcomes.
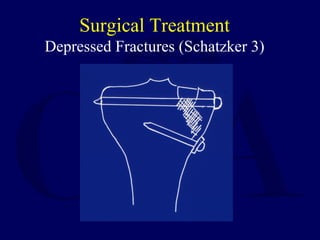
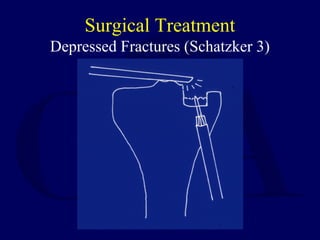
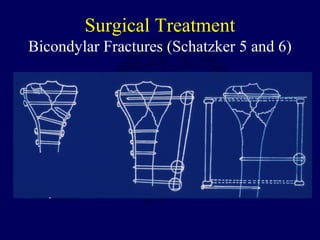
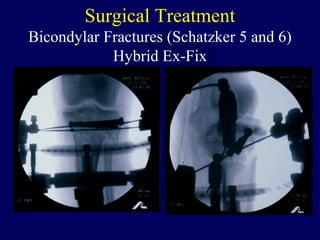
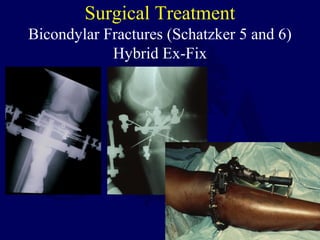
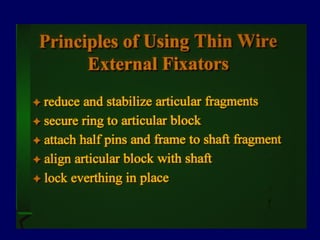
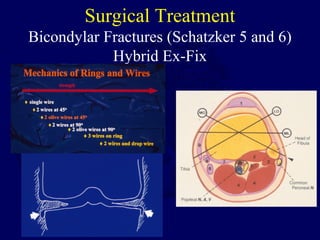
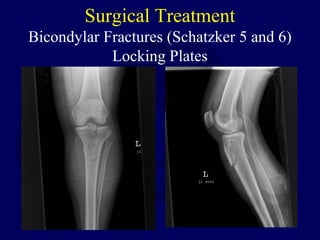
2) Surgical treatment may involve open reduction and internal fixation with plates and screws or less invasive options like percutaneous plating and hybrid external fixation to minimize soft tissue disruption.
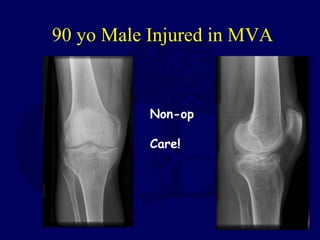
3) Patient factors like age, comorbidities, and the specific fracture pattern help determine the best treatment which can range from non-operative management to internal fixation, external fixation, or a combination approach.






















































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
