This document discusses the history and treatment of distal radius fractures. Some key points:
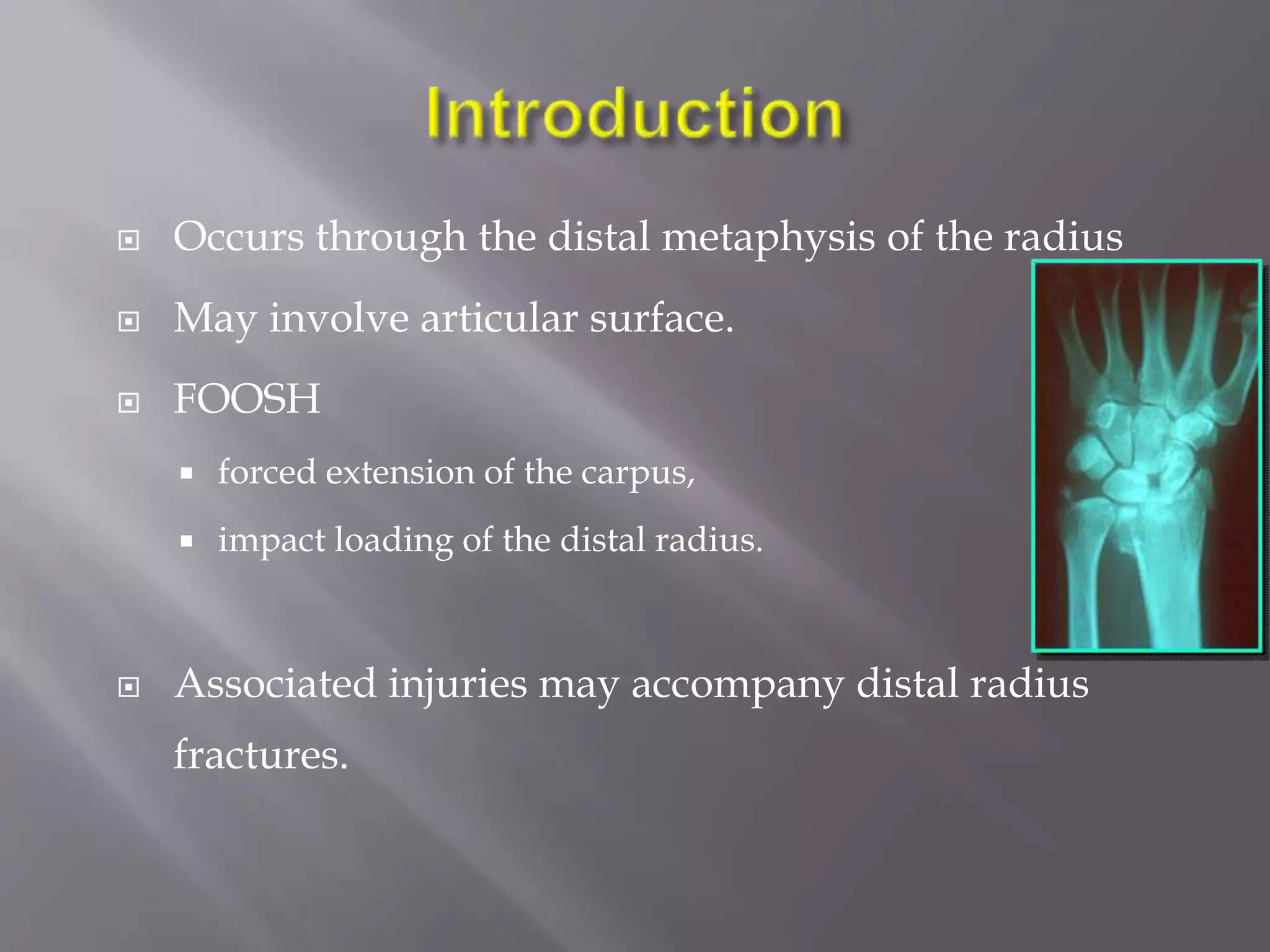
- Distal radius fractures are common injuries that were first recognized in the late 18th century, with descriptions of injury patterns evolving over the 19th century.
- Treatment has progressed from casting to external fixation to various internal fixation methods like dorsal, volar, and combined plating approaches.
- Factors like fracture pattern, displacement, comminution, and articular involvement help determine appropriate treatment, whether closed reduction or open reduction with internal fixation.
- The goal of treatment is to restore normal anatomy, allow early motion, and avoid complications like malunion.