Downloaded 436 times







![DISI
When the scaphoid is
destabilized by fracture or
scapholunate ligament
disruption, the lunate and
triquetrum assume a position
of excessive dorsiflexion
(dorsal intercalated segmental
instability [DISI] ) and the
scapholunate angle becomes
abnormally high (>70
degrees).](https://image.slidesharecdn.com/periluntedisloc-171201133850/85/Perilunate-dislocations-10-320.jpg)
![VISI
When the triquetrum is
destabilized (usually by
disruption of the
lunotriquetral ligament
complex), the opposite
pattern (volar intercalated
segmental instability [VISI] )
is seen as the lunate
(intercalated segment) volar
flexes.](https://image.slidesharecdn.com/periluntedisloc-171201133850/85/Perilunate-dislocations-11-320.jpg)

































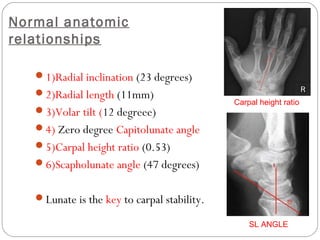
1) The document discusses various carpal dislocations including perilunate dislocations and fractures, scapholunate dissociation, and their anatomy, mechanisms of injury, clinical features, imaging, and management. 2) Perilunate dislocations are high energy injuries that commonly involve disruption of the scapholunate ligament followed by other ligaments and can be classified using the Mayfield classification system. Management involves early closed reduction and surgery including open reduction, ligament repair and fixation. 3) Scapholunate dissociation is an important cause of carpal instability that can lead to DISI deformity if left untreated. The scapholunate ligament maintains carpal stability and its anatomy and biomechan



































































