Downloaded 157 times
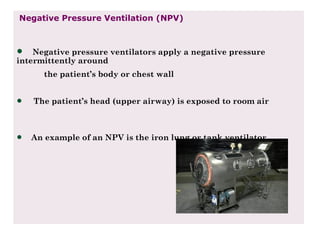





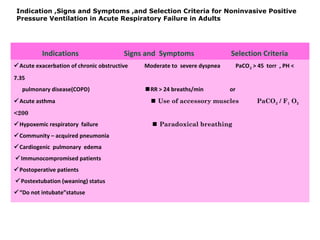
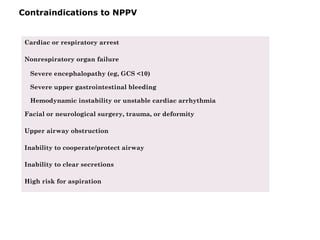




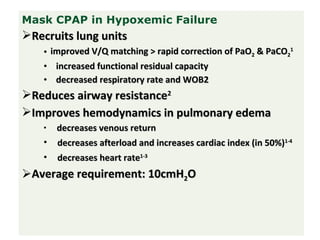







The document discusses non-invasive ventilation (NIV) techniques, highlighting benefits such as reduced need for intubation, better patient comfort, and decreased risk of complications compared to invasive methods. It outlines different types of NIV, including negative pressure ventilation, noninvasive positive pressure ventilation (NPPV), CPAP, and BiPAP, along with their indications, contraindications, and success indicators. Additionally, the document provides guidelines for initiating NPPV and criteria for transitioning to invasive ventilation if necessary.





























































































