Downloaded 122 times
![Aortic Regurgitation: overview
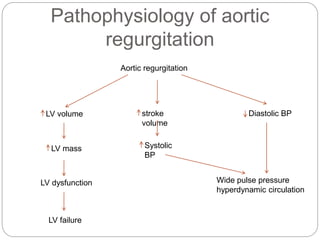
AR is a condition due to inadequate closure of
the aortic valve leaflets leading to abnormal
retrograde flow of blood through the aortic
valve during cardiac diastole.
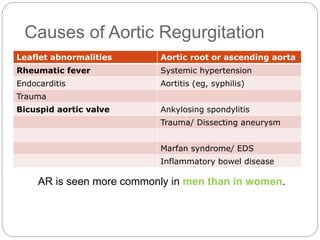
It can be induced either by damage to and
dysfunction of the aortic valve leaflets or by
distortion or dilatation of the aortic root and
ascending aorta
In the developing world, the most common cause
of AR is rheumatic heart disease. However, in
developed countries, AR is most often due to
aortic root dilation or a congenital bicuspid
aortic valve .[1]](https://image.slidesharecdn.com/aorticstenosis-170329092516/85/Aortic-stenosis-16-320.jpg)

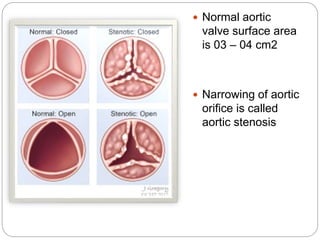
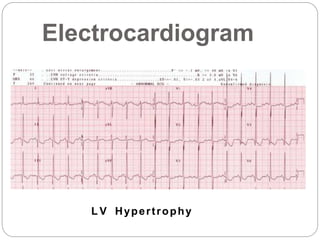
This document discusses aortic stenosis and aortic regurgitation. It defines aortic stenosis as a narrowing of the aortic valve opening, with common causes being a bicuspid aortic valve, calcification, or rheumatic heart disease. Symptoms include angina, syncope, and dyspnea. Diagnosis involves echocardiography. Treatment options are balloon valvuloplasty or valve replacement. Aortic regurgitation is defined as retrograde blood flow through the aortic valve during diastole. Common causes are rheumatic fever, hypertension, or a bicuspid valve. Symptoms progress from palpitations to dyspnea. Physical exam may reveal a wide pulse pressure.




















































































