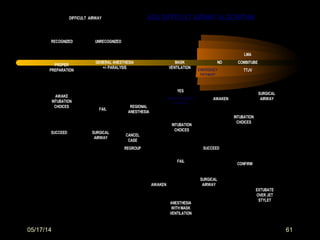
This document discusses the management of difficult airways. It begins with definitions of difficult airway situations according to the American Society of Anesthesiologists. It then discusses the prevalence, causes, and basic airway evaluation including the "Lemon Law" assessment. Management plans for anticipated difficult airways including having alternative intubation techniques ("Plan B" and "C") are covered. A gallery of tools for difficult intubation including different laryngoscope blades, supraglottic airways, and fiberoptic intubation are presented. The document concludes with discussions on unexpected difficult airways, the ASA difficult airway algorithm, and emphasizes being prepared with alternative intubation methods.


























































![Anesthesia_for_Airway_management_and_Difficult_airway_Algorithmss[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforairwaymanagementanddifficultairwayalgorithmss11-250722203414-f94048f1-thumbnail.jpg?width=640&height=640&fit=bounds)



















































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)