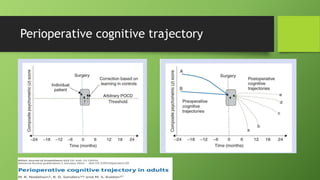
Postoperative cognitive dysfunction (POCD) is a cognitive impairment observed in elderly patients following major surgeries, characterized by memory loss and decreased concentration without affecting consciousness. It affects approximately 40% of patients over 60 at discharge, with varying incidences based on surgery type and individual risk factors. Prevention strategies include preoperative optimization, careful anesthesia management, and postoperative interventions to support cognitive function.











![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)


























































