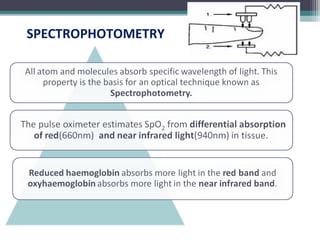
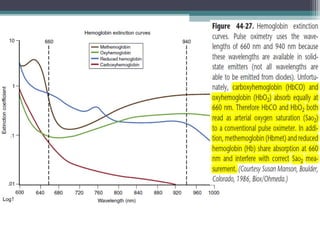
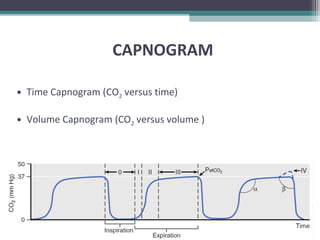
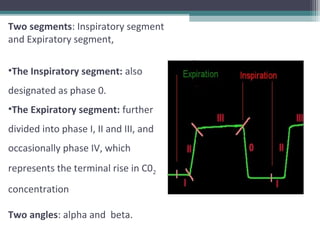
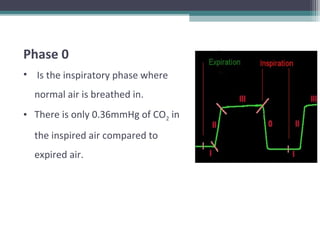
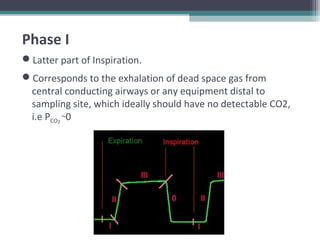
This document provides information on pulse oximetry and capnography. It discusses the history and development of pulse oximetry, how it works using spectrophotometry and plethysmography, different probe sites, standards, uses, limitations and new developments. It also briefly introduces capnography and defines key terms like capnometry, capnometer and capnograph.
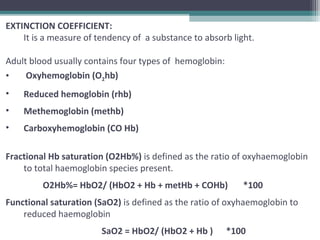
![O2 content of arterial blood is,
CaO2 = Oxygen bound to hemoglobin + O2 dissolved in plasma
CaO2 = [1.36 × Hb × HbO % (SpO2)] + [0.003 × PaO2].
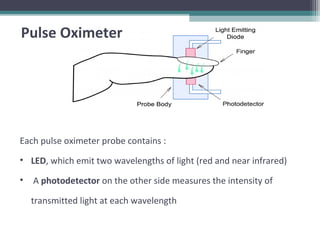
Pulse oximeter provides a non
invasive measurement of
arterial hemoglobin
saturation, a variable that is
directly related to oxygen
content of arterial
blood..](https://image.slidesharecdn.com/pulseoximetrycapnographymain-190624113859/85/Pulse-oximetry-capnography-14-320.jpg)



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











