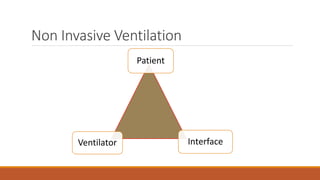
The presentation by Dr. Somnath Longani focuses on non-invasive ventilation (NIV), including its indications, contraindications, and the different types of ventilators and modes available. It details how to assess the need for NIV, select appropriate interfaces, and initiate therapy while addressing potential complications and monitoring strategies. The document emphasizes the importance of patient selection, training, and careful adjustment of ventilator settings to ensure successful outcomes with NIV.